

Minimally Invasive Beaded Electrosurgical Dissectors, Basic Science, and Pilot Studies
- PMID: 38938927
- PMCID: PMC11210070
- DOI: 10.1093/asjof/ojae034
Minimally Invasive Beaded Electrosurgical Dissectors, Basic Science, and Pilot Studies
Abstract
Background: Minimally invasive beaded electrosurgical dissectors ("BEED devices") provide simultaneous sharp dissection, blunt dissection, and electrosurgical coagulation while performing 100 cm2 porcine tissue plane dissections in 0.8 to 3 min with minimal bleeding and no perforations.
Objectives: The aim of the study was to report the basic science and potential clinical applications and to video document the speed and quality of planar dissections in in vivo and ex vivo porcine models with thermal damage quantified by thermal and histopathologic measurements. Additionally, in vivo porcine specimens were followed for 90 days to show whether adverse events occurred on a gross or macroscopic basis, as evidenced by photography, videography, physical examination, and dual ultrasonography.
Methods: Ex vivo porcine models were subjected to 20, 30, and 50 W in single-stroke passages with BEED dissectors (granted FDA 510(k) clearance (K233002)) with multichannel thermocouple, 3 s delay recordation combined with matching hematoxylin and eosin (H&E) histopathology. In vivo porcine models were subjected to eight 10 × 10 cm dissections in each of 2 subjects at 20, 30, and 50 W and evaluated periodically until 90 days, wherein histopathology for H&E, collagen, and elastin was taken plus standard and Doppler ultrasounds prior to euthanasia.
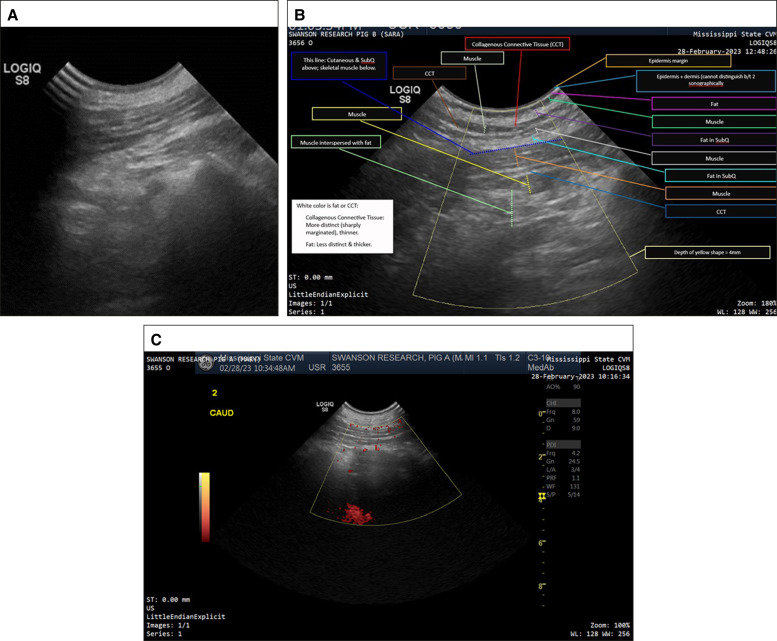
Results: Five to 8 mm width dissectors were passed at 1 to 2 cm/s in ex vivo models (1-10 cm/s in vivo models) with an average temperature rise of 5°C at 50 W. Clinically evidenced seromas occurred in the undressed, unprotected wounds, and resolved well prior to 90 days, as documented by ultrasounds and histopathology.
Conclusions: In vivo and ex vivo models demonstrated thermal values that were below levels known to damage subcutaneous adipose tissue or skin. Tissue histopathology confirmed healing parameters while Doppler ultrasound demonstrated normal blood flow in posttreatment tissues.
© The Author(s) 2024. Published by Oxford University Press on behalf of The Aesthetic Society.
Figures








References
Publication types
LinkOut - more resources
Full Text Sources