

Cumulative In-Hospital Costs Associated With Single-Ventricle Palliation
- PMID: 38939312
- PMCID: PMC11198056
- DOI: 10.1016/j.jacadv.2022.100029
Cumulative In-Hospital Costs Associated With Single-Ventricle Palliation
Abstract
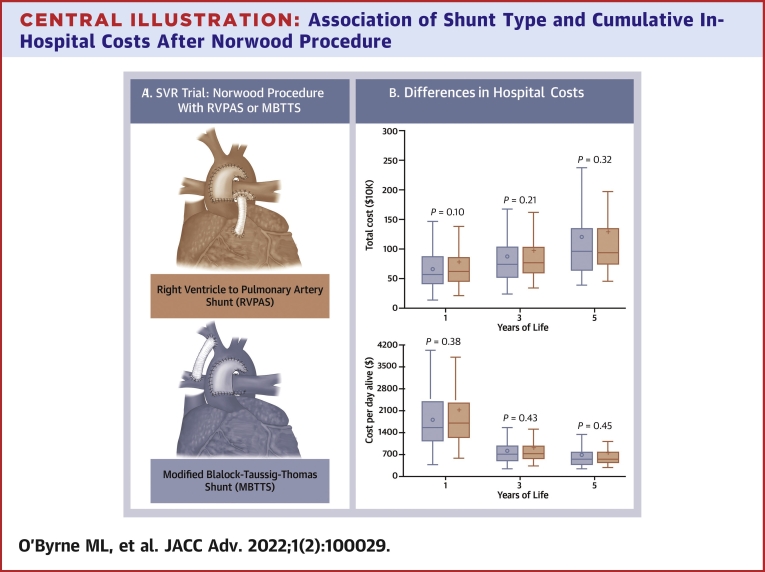
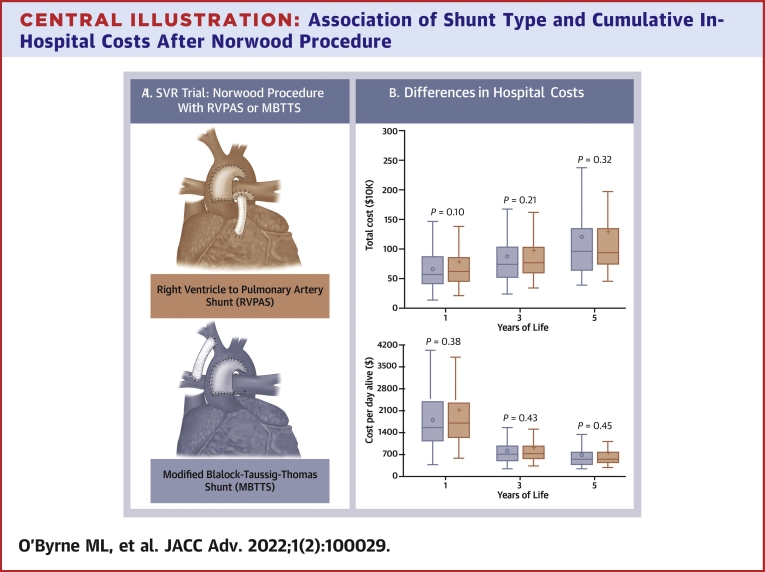
Background: In the SVR (Single Ventricle Reconstruction) Trial, 1-year survival in recipients of right ventricle to pulmonary artery shunts (RVPAS) was superior to that in those receiving modified Blalock-Taussig-Thomas shunts (MBTTS), but not in subsequent follow-up. Cost analysis is an expedient means of evaluating value and morbidity.
Objectives: The purpose of this study was to evaluate differences in cumulative hospital costs between RVPAS and MBTTS.
Methods: Clinical data from SVR and costs from Pediatric Health Information Systems database were combined. Cumulative hospital costs and cost-per-day-alive were compared serially at 1, 3, and 5 years between RVPAS and MBTTS. Potential associations between patient-level factors and cost were explored with multivariable models.
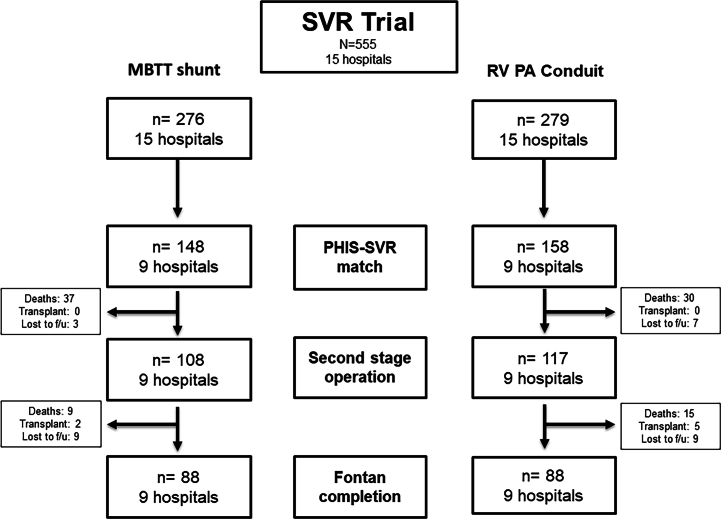
Results: In total, 303 participants (55% of the SVR cohort) from 9 of 15 sites were studied (48% MBTTS). Observed total costs at 1 year were lower for MBTTS ($701,260 ± 442,081) than those for RVPAS ($804,062 ± 615,068), a difference that was not statistically significant (P = 0.10). Total costs were also not significantly different at 3 and 5 years (P = 0.21 and 0.32). Similarly, cost-per-day-alive did not differ significantly for either group at 1, 3, and 5 years (all P > 0.05). In analyses of transplant-free survivors, total costs and cost-per-day-alive were higher for RVPAS at 1 year (P = 0.05 for both) but not at 3 and 5 years (P > 0.05 for all). In multivariable models, aortic atresia and prematurity were associated with increased cost-per-day-alive across follow-up (P < 0.05).
Conclusions: Total costs do not differ significantly between MBTTS and RVPAS. The magnitude of longitudinal costs underscores the importance of efforts to improve outcomes in this vulnerable population.
Keywords: economic analysis; hypoplastic left heart syndrome; outcomes research; pediatrics.
© 2022 The Authors.
Conflict of interest statement
The SVR trial was funded by the Pediatric Heart Network/10.13039/100000050National Heart, Lung, and Blood Institute (HL068269, HL068270, HL068279, HL068281, HL068285, HL068288, HL068290, HL068292, and HL085057). Dr O'Byrne received support from 10.13039/100000050NHLBI (K23 HL130420-01). The project also received assistance from The Pediatric Heart Network’s Integrated CARDiac Data and Outcomes Collaborative (iCARD). The Pediatric Heart Network Ancillary Studies Committee and Single Ventricle Reconstruction Trial Committee reviewed the proposed research and manuscript for appropriateness but did not participate in the drafting of the paper. The views expressed are solely of the authors and do not reflect those of the funders and other supporting groups. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.PERSPECTIVESCOMPETENCY IN MEDICAL KNOWLEDGE: Costs (which are reflective of morbidity) overall did not differ between participants randomized to a Blalock-Taussig-Thomas shunt and those to a RVPAS. However, analysis of survivors suggests that the cost of living with a RVPAS is higher, consistent with higher reintervention rates, while higher mortality rates increased costs of the Blalock-Taussig-Thomas shunt strategy. Differences in cost were derived from differences in the first year of life where the majority of total costs were accrued. Efforts to improve care should focus on improving outcomes in this period. TRANSLATIONAL OUTLOOK: Although it did not reveal significant differences in costs between shunt types, this analysis of the SVR trial leads to a better understanding of the economic and medical impact of operative palliation for single ventricle heart disease.
Figures
References
-
- O'Brien S.M., Clarke D.R., Jacobs J.P., et al. An empirically based tool for analyzing mortality associated with congenital heart surgery. J Thorac Cardiovasc Surg. 2009;138:1139–1153. - PubMed
-
- Menon S.C., Erickson L.K., McFadden M., Miller D.V. Effect of ventriculotomy on right-ventricular remodeling in hypoplastic left heart syndrome: a histopathological and echocardiography correlation study. Pediatr Cardiol. 2013;34:354–363. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
