

Treatment Intensity for the Management of Cardiogenic Shock: Comparison Between STEMI and Non-STEMI
- PMID: 38939594
- PMCID: PMC11198573
- DOI: 10.1016/j.jacadv.2023.100314
Treatment Intensity for the Management of Cardiogenic Shock: Comparison Between STEMI and Non-STEMI
Abstract
Background: Cardiogenic shock is a leading cause of mortality in patients with acute myocardial infarction.
Objectives: The authors sought to compare clinical characteristics, hospital trajectory, and drug and device use between patients with ST-segment elevation myocardial infarction-related cardiogenic shock (STEMI-CS) and those without (non-ST-segment elevation myocardial infarction complicated by cardiogenic shock [NSTEMI-CS]).
Methods: We analyzed data from 1,110 adult admissions with cardiogenic shock complicating acute myocardial infarction (AMI-CS) across 17 centers within Cardiogenic Shock Working Group. The primary end point was in-hospital mortality.
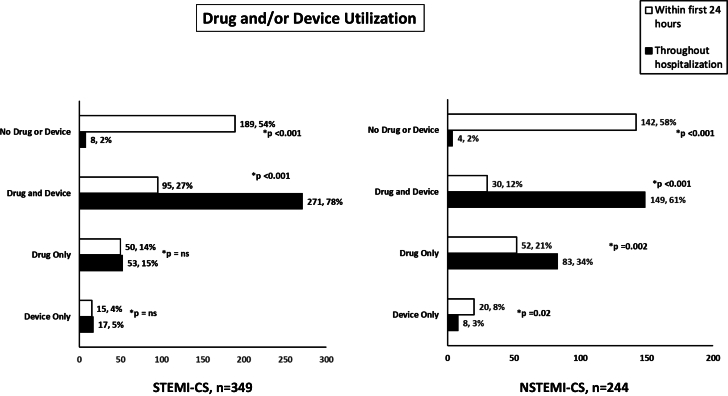
Results: Our study included 1,110 patients with AMI-CS, of which 731 (65.8%) had STEMI-CS and 379 (34.2%) had NSTEMI-CS. Most patients were male (STEMI-CS: 71.6%, NSTEMI-CS: 66.5%) and White (STEMI-CS: 53.8%, NSTEMI-CS: 64.1%). In-hospital mortality was 41% and was similar among patients with STEMI-CS and NSTEMI-CS (43% vs 39%, P = 0.23). Patients with out-of-hospital cardiac arrest had higher in-hospital mortality in patients with NSTEMI-CS (63% vs 36%, P = 0.006) as compared to patients with STEMI-CS (52% vs 41%, P = 0.16). Similar results were observed for in-hospital cardiac arrest in patients with STEMI-CS (63% vs 33%, P < 0.001) and NSTEMI-CS (60% vs 32%, P < 0.001). Only 27% of patients with STEMI-CS and 12% of NSTEMI-CS received both a drug and temporary mechanical circulatory support device during the first 24 hours, which increased to 78% and 61%, respectively, throughout the course of the hospitalization (P < 0.001 for both).
Conclusions: Despite increasing use of inotropic and vasoactive support and mechanical circulatory support throughout the hospitalization, both patients with STEMI-CS and NSTEMI-CS remain at increased risk for in-hospital mortality. Randomized controls trials are needed to elucidate whether timing and sequence of escalation of support improves outcomes in patients with AMI-CS.
Keywords: acute myocardial infarction; cardiogenic shock; heart failure.
© 2023 The Authors.
Conflict of interest statement
This work was supported by a 10.13039/100000002NIH RO1 grants to Dr Kapur (R01HL139785-01; R01HL159089-01) and institutional grants from 10.13039/100020297Abiomed Inc, 10.13039/100008497Boston Scientific Inc, 10.13039/100001316Abbott Laboratories, Getinge Inc, and 10.13039/100013410LivaNova Inc to Tufts Medical Center. Sponsors had no input on collection, analysis, and interpretation of the data, nor in the preparation, review, or approval of the manuscript. Dr Kapur has received consulting honoraria and institutional grant support from Abbott Laboratories, Abiomed Inc, Boston Scientific, Medtronic, LivaNova, Getinge, and Zoll. Dr Hernandez-Montfort is a consultant for Abiomed Inc. Dr Abraham is a consultant for Abbott Laboratories and Abiomed Inc. Dr Burkhoff has received support from consulting services provided from Abiomed Inc. to Cardiovascular Research Foundation. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures





References
LinkOut - more resources
Full Text Sources
