

Pulmonary cryptococcosis in non-HIV-infected individuals: HRCT characteristics in 58 patients
- PMID: 38941424
- PMCID: PMC11466118
- DOI: 10.1097/MD.0000000000038671
Pulmonary cryptococcosis in non-HIV-infected individuals: HRCT characteristics in 58 patients
Abstract
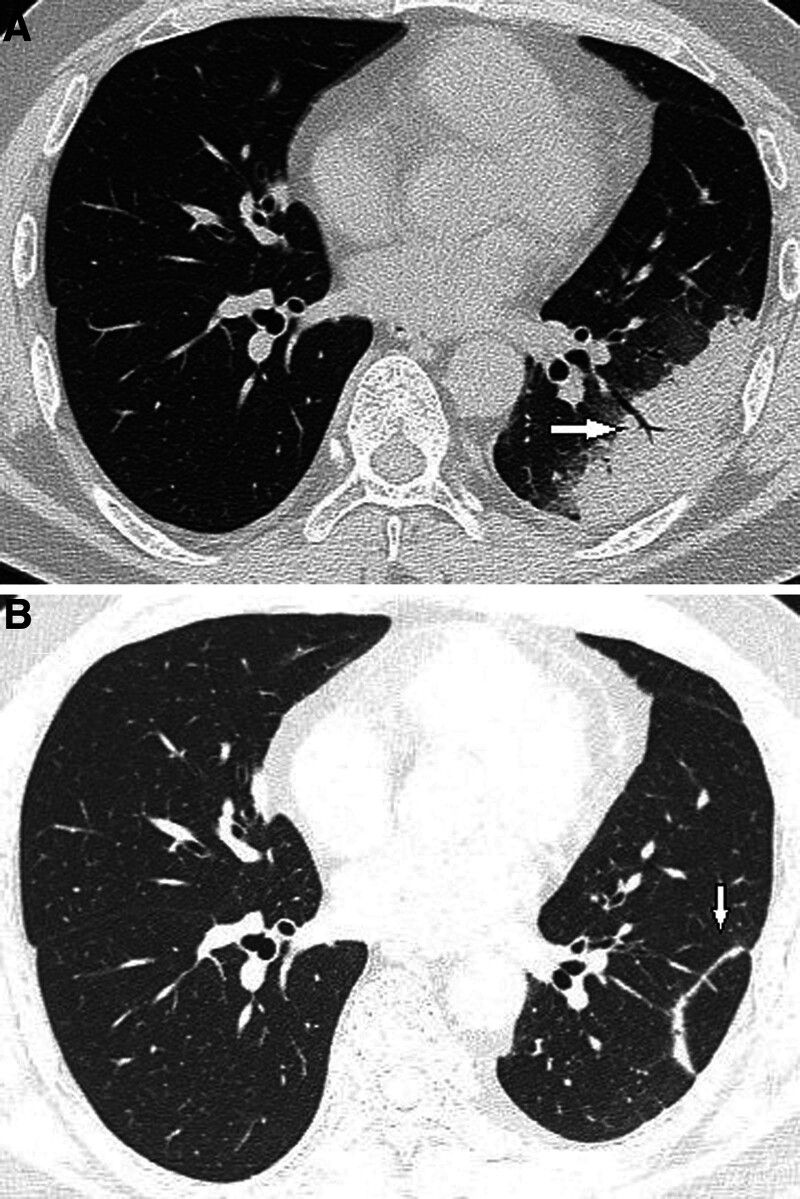
The aim of this study is to delineate the distinctive high-resolution computed tomography features of pulmonary cryptococcosis in non-HIV-infected patients. This retrospective analysis encompasses high-resolution computed tomography scans from 58 patients with histologically confirmed pulmonary cryptococcosis, focusing on the diagnostic challenges and the factors that lead to misdiagnosis. Analysis of computed tomography scans from these patients indicated that nodular or mass-like presentations were evident in 32 cases (55.2%), consolidation presentations in 7 cases (12.1%), and mixed presentations in 19 cases (32.8%). Lesions were predominantly located in the lower lobes of the lungs (40 cases, 69.0%) and in peripheral zones (55 cases, 94.8%). Notable radiographic signs included the presence of the burr sign in 55 cases (94.8%), lobulation sign in 53 cases (91.4%), halo sign in 53 cases (91.4%), and air bronchogram in 46 cases (79.0%). Moreover, 24 cases (41.4%) exhibited necrosis or cavitation, mediastinal lymphadenopathy was noted in 6 cases (10.3%), and pleural effusion was present in 5 cases (8.6%). Lesions were devoid of calcification. Pulmonary cryptococcosis ought to be contemplated in the differential diagnosis when computed tomography imaging exhibits patterns including, but not limited to, lower lobe and peripheral distribution, a broad base abutting the pleura, clustered growth with a propensity for fusion, air bronchogram within lesions, and peripheral halo sign.
Copyright © 2024 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures


Similar articles
-
Pulmonary cryptococcosis: comparison of CT findings in immunocompetent and immunocompromised patients.Acta Radiol. 2015 Apr;56(4):447-53. doi: 10.1177/0284185114529105. Epub 2014 Apr 22. Acta Radiol. 2015. PMID: 24757183
-
[Retrospective analysis of 117 cases of pulmonary cryptococcosis].Zhonghua Jie He He Hu Xi Za Zhi. 2016 Nov 12;39(11):862-865. doi: 10.3760/cma.j.issn.1001-0939.2016.11.008. Zhonghua Jie He He Hu Xi Za Zhi. 2016. PMID: 27852362 Chinese.
-
[CT Characteristics of Consolidation Type of Pulmonary Cryptococcosis in Immunocompetent Patients].Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2021 Apr 28;43(2):216-221. doi: 10.3881/j.issn.1000-503X.12736. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2021. PMID: 33966701 Chinese.
-
Computed tomography features of COVID-19 in children: A systematic review and meta-analysis.Medicine (Baltimore). 2021 Sep 24;100(38):e22571. doi: 10.1097/MD.0000000000022571. Medicine (Baltimore). 2021. PMID: 34559092 Free PMC article.
-
Pleural fluid secondary to pulmonary cryptococcal infection: a case report and review of the literature.BMC Infect Dis. 2019 Aug 12;19(1):710. doi: 10.1186/s12879-019-4343-2. BMC Infect Dis. 2019. PMID: 31405376 Free PMC article. Review.
Cited by
-
Clinicopathological Analysis of 60 Cases of Pulmonary Cryptococcosis.Int J Gen Med. 2025 Jun 17;18:3207-3214. doi: 10.2147/IJGM.S525789. eCollection 2025. Int J Gen Med. 2025. PMID: 40547348 Free PMC article.
-
Clinical-imaging diversity of exudative pulmonary cryptococcosis with different immune states.Sci Rep. 2025 Jul 14;15(1):25346. doi: 10.1038/s41598-025-10807-3. Sci Rep. 2025. PMID: 40659736 Free PMC article.
References
-
- Brizendine KD, Baddley JW, Pappas PG. Pulmonary cryptococcosis. Semin Respir Crit Care Med. 2011;32:727–34. - PubMed
