

Nipocalimab, an anti-FcRn monoclonal antibody, in participants with moderate to severe active rheumatoid arthritis and inadequate response or intolerance to anti-TNF therapy: results from the phase 2a IRIS-RA study
- PMID: 38942592
- PMCID: PMC11227837
- DOI: 10.1136/rmdopen-2024-004278
Nipocalimab, an anti-FcRn monoclonal antibody, in participants with moderate to severe active rheumatoid arthritis and inadequate response or intolerance to anti-TNF therapy: results from the phase 2a IRIS-RA study
Abstract
Objectives: To investigate the efficacy, safety, pharmacokinetics and pharmacodynamics of nipocalimab in participants with moderate to severe active rheumatoid arthritis (RA) and inadequate response or intolerance to ≥1 antitumour necrosis factor agent.
Methods: In this phase 2a study, participants with RA seropositive for anticitrullinated protein antibodies (ACPA) or rheumatoid factors were randomised 3:2 to nipocalimab (15 mg/kg intravenously every 2 weeks) or placebo from Weeks 0 to 10. Efficacy endpoints (primary endpoint: change from baseline in Disease Activity Score 28 using C reactive protein (DAS28-CRP) at Week 12) and patient-reported outcomes (PROs) were assessed through Week 12. Safety, pharmacokinetics and pharmacodynamics were assessed through Week 18.
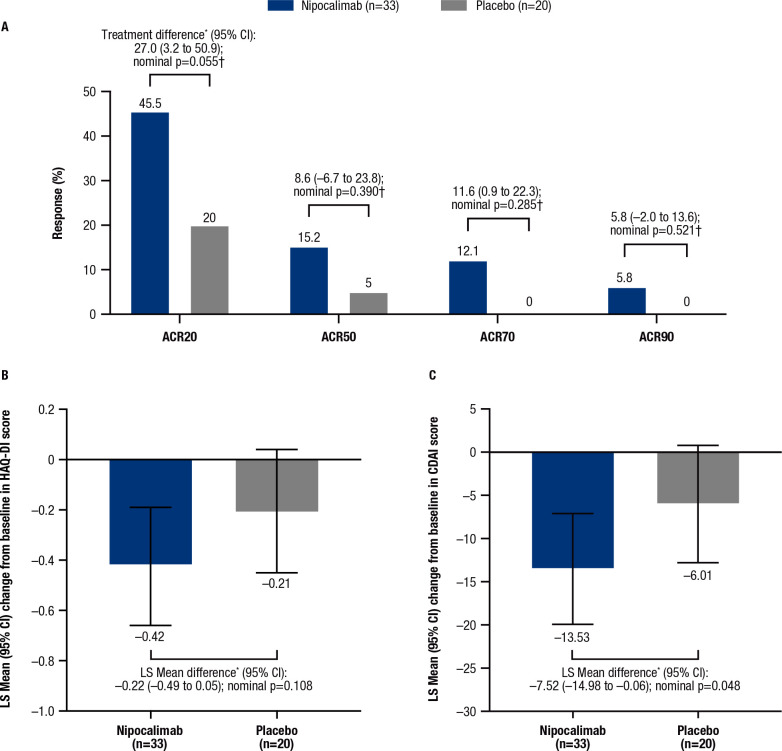
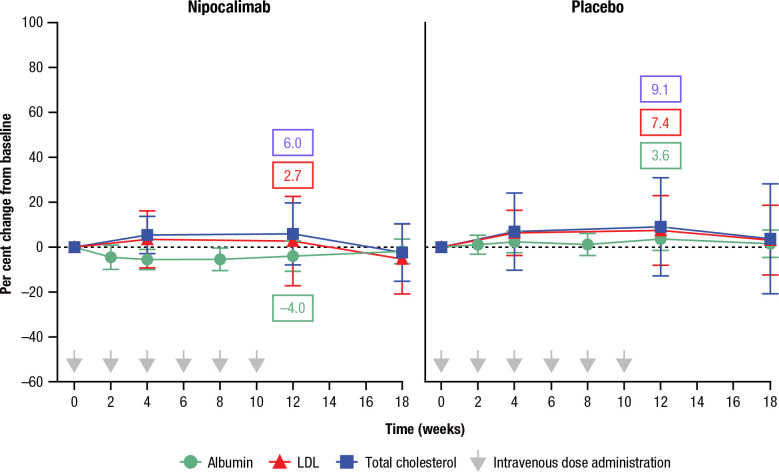
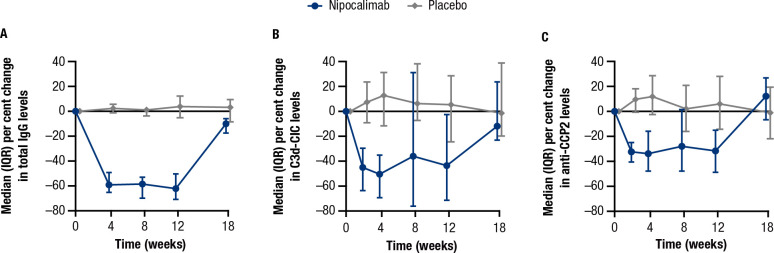
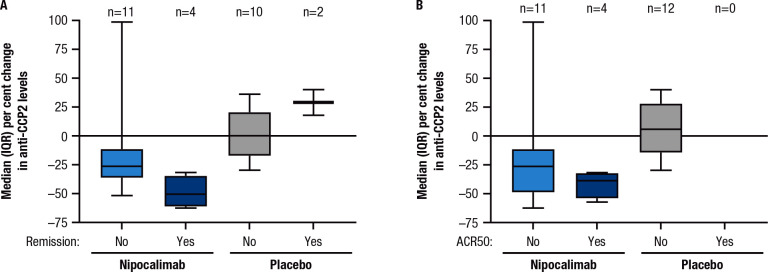
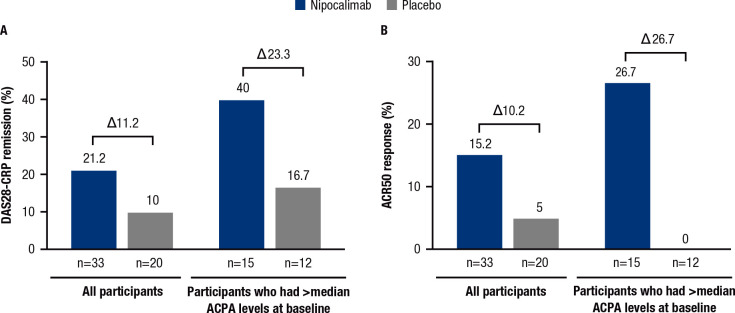
Results: 53 participants were enrolled (nipocalimab/placebo, n=33/20). Although the primary endpoint did not reach statistical significance for nipocalimab versus placebo, a numerically higher change from baseline in DAS28-CRP at Week 12 was observed (least squares mean (95% CI): -1.03 (-1.66 to -0.40) vs -0.58 (-1.24 to 0.07)), with numerically higher improvements in all secondary efficacy outcomes and PROs. Serious adverse events were reported in three participants (burn infection, infusion-related reaction and deep vein thrombosis). Nipocalimab significantly and reversibly reduced serum immunoglobulin G, ACPA and circulating immune complex levels but not serum inflammatory markers, including CRP. ACPA reduction was associated with DAS28-CRP remission and 50% response rate in American College of Rheumatology (ACR) criteria; participants with a higher baseline ACPA had greater clinical improvement.
Conclusions: Despite not achieving statistical significance in the primary endpoint, nipocalimab showed consistent, numerical efficacy benefits in participants with moderate to severe active RA, with greater benefit observed for participants with a higher baseline ACPA.
Trial registration number: NCT04991753.
Keywords: Anti-Citrullinated Protein Antibodies; Arthritis, Rheumatoid; Patient Reported Outcome Measures; Rheumatoid Factor.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: PCT serves on a DSMB for Immunovant; serves as a consultant for AbbVie, Aqtual, Biogen, Eli Lilly, Fresenius, Galapagos, Gilead Sciences, GSK, Janssen, Nordic Pharma, Pfizer, Sanofi and UCB and receives grants/research support from Galapagos. GS has no conflict of interest. TWJH receives grants/research support from Janssen. QW, FI, BZ, SGL, JSBS, YX, JHL, RAP, MJL, KM, HD, RRC, CSK, CAC, SG and KF are employees of Janssen and may hold stock in Johnson & Johnson.
Figures

References
-
- Wolfe F, Hawley DJ, Wilson K. The prevalence and meaning of fatigue in rheumatic disease. J Rheumatol 1996;23:1407–17. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous