

Multiple myeloma: 2024 update on diagnosis, risk-stratification, and management
- PMID: 38943315
- PMCID: PMC11404783
- DOI: 10.1002/ajh.27422
Multiple myeloma: 2024 update on diagnosis, risk-stratification, and management
Abstract
Disease overview: Multiple myeloma accounts for approximately 10% of hematologic malignancies.
Diagnosis: The diagnosis requires ≥10% clonal bone marrow plasma cells or a biopsy proven plasmacytoma plus evidence of one or more multiple myeloma defining events (MDE): CRAB (hypercalcemia, renal failure, anemia, or lytic bone lesions) attributable to the plasma cell disorder, bone marrow clonal plasmacytosis ≥60%, serum involved/uninvolved free light chain (FLC) ratio ≥100 (provided involved FLC is ≥100 mg/L and urine monoclonal protein is ≥200 mg/24 h), or >1 focal lesion on magnetic resonance imaging.
Risk stratification: The presence of del(17p), t(4;14), t(14;16), t(14;20), gain 1q, del 1p, or p53 mutation is considered high-risk multiple myeloma. Presence of any two high risk factors is considered double-hit myeloma; three or more high risk factors is triple-hit myeloma.
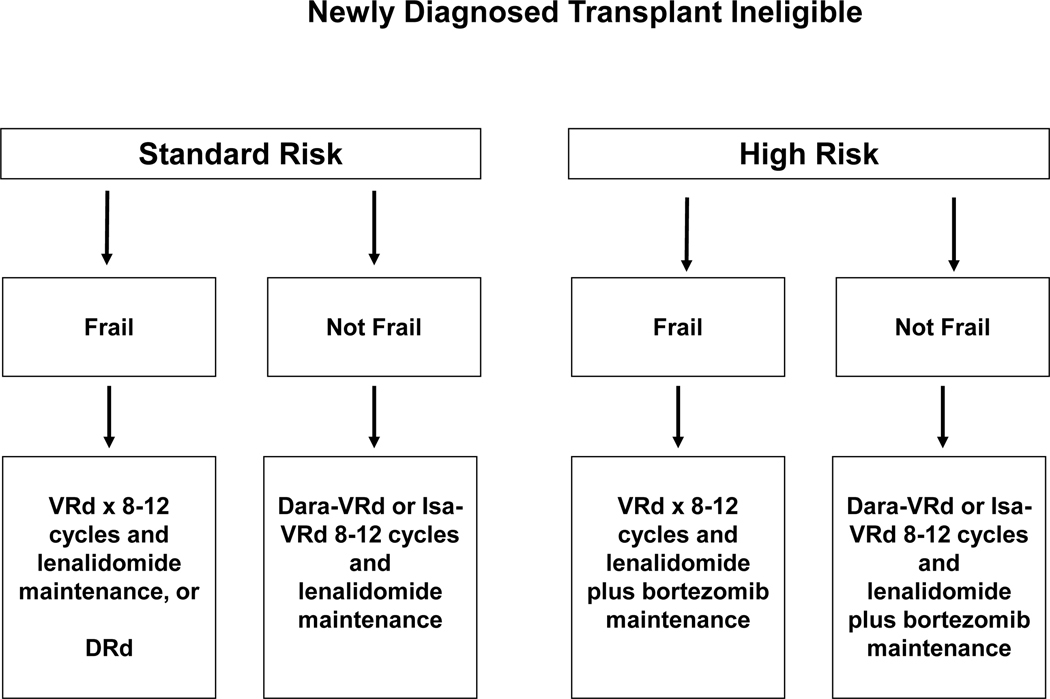
Risk-adapted initial therapy: In patients who are candidates for autologous stem cell transplantation, induction therapy consists of anti-CD38 monoclonal antibody plus bortezomib, lenalidomide, dexamethasone (VRd) followed by autologous stem cell transplantation (ASCT). Selected standard risk patients can delay transplant until first relapse. Frail patients who not candidates for transplant are treated with VRd for approximately 8-12 cycles followed by maintenance or alternatively with daratumumab, lenalidomide, dexamethasone (DRd) until progression.
Maintenance therapy: Standard risk patients need lenalidomide maintenance, while bortezomib plus lenalidomide maintenance is needed for high-risk myeloma.
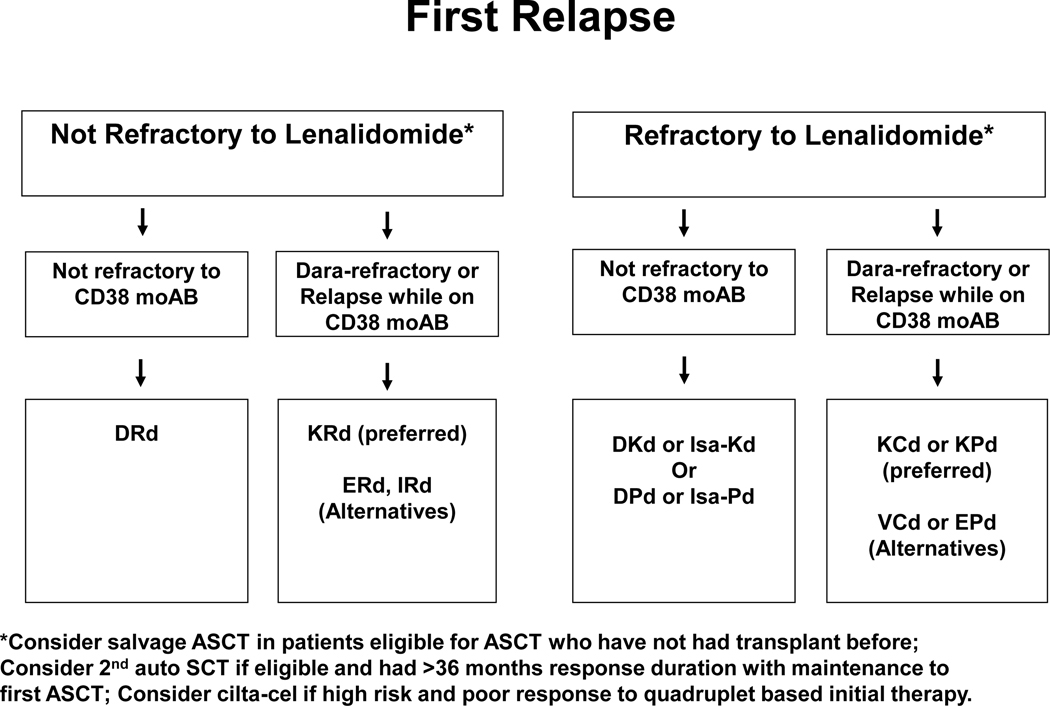
Management of relapsed disease: A triplet regimen is usually needed at relapse, with the choice of regimen varying with each successive relapse. Chimeric antigen receptor T (CAR-T) cell therapy and bispecific antibodies are additional options.
© 2024 Wiley Periodicals LLC.
Conflict of interest statement
Disclosure of Conflicts of Interest
SVR declares no conflict of interest.
Conflict of interest: No conflicts of interest to be disclosed.
Figures


References
-
- Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group Updated Criteria for the Diagnosis of Multiple Myeloma. Lancet Oncol 2014;15(12):e538–548. (http://linkinghub.elsevier.com/retrieve/pii/S1470204514704425). - PubMed
-
- Kyle RA, Therneau TM, Rajkumar SV, Larson DR, Plevak MF, Melton LJ 3rd. Incidence of multiple myeloma in Olmsted County, Minnesota: Trend over 6 decades. Cancer 2004;101(11):2667–74. - PubMed
-
- Kyle RA, Gertz MA, Witzig TE, et al. Review of 1,027 patients with newly diagnosed multiple myeloma. Mayo Clinic Proc 2003;78:21–33. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous