

Comparison of Early Fungicidal Activity and Mortality Between Daily Liposomal Amphotericin B and Daily Amphotericin B Deoxycholate for Cryptococcal Meningitis
- PMID: 38943665
- PMCID: PMC11797393
- DOI: 10.1093/cid/ciae326
Comparison of Early Fungicidal Activity and Mortality Between Daily Liposomal Amphotericin B and Daily Amphotericin B Deoxycholate for Cryptococcal Meningitis
Abstract
Background: Limited data exist on the antifungal activity of daily liposomal amphotericin B with flucytosine induction regimens for cryptococcal meningitis, which are recommended in high-income countries. Liposomal amphotericin B monotherapy at 3 mg/kg previously failed to meet noninferiority criteria compared to amphotericin B deoxycholate in its registrational clinical trial. We aimed to compare the quantitative antifungal activity and mortality between daily amphotericin B deoxycholate and daily liposomal amphotericin B among persons with human immunodeficiency virus (HIV)-related cryptococcal meningitis receiving adjunctive flucytosine 100 mg/kg/day.
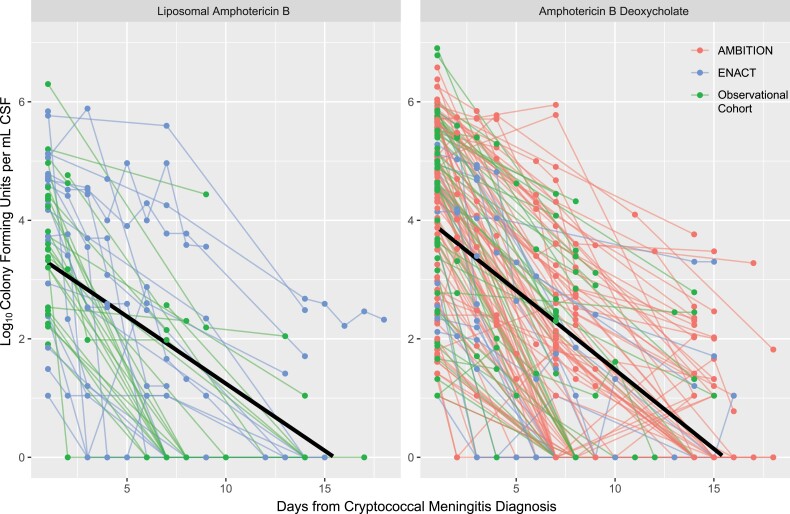
Methods: We analyzed data from 3 clinical studies involving participants with HIV-associated cryptococcal meningitis receiving either daily liposomal amphotericin B at 3 mg/kg/day with flucytosine (n = 94) or amphotericin B deoxycholate at 0.7-1.0 mg/kg/day with flucytosine (n = 404) as induction therapy. We compared participant baseline characteristics, cerebrospinal fluid (CSF) early fungicidal activity (EFA), and 10-week mortality.
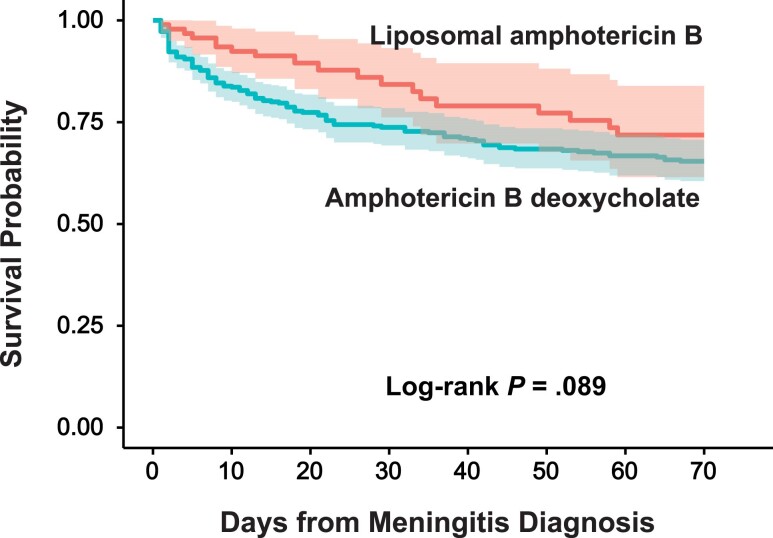
Results: We included 498 participants in this analysis, of whom 201 had available EFA data (n = 46 liposomal amphotericin B; n = 155 amphotericin B deoxycholate). Overall, there is no statistical evidence that the antifungal activity of liposomal amphotericin B (mean EFA, 0.495 [95% confidence interval {CI}, .355-.634] log10 colony-forming units [CFU]/mL/day) differ from amphotericin B deoxycholate (mean EFA, 0.402 [95% CI, .360-.445] log10 CFU/mL) (P = .13). Mortality at 10 weeks trended lower for liposomal amphotericin B (28.2%) versus amphotericin B deoxycholate (34.6%) but was not statistically different when adjusting for baseline characteristics (adjusted hazard ratio, 0.74 [95% CI, .44-1.25]; P = .26).
Conclusions: Daily liposomal amphotericin B induction demonstrated a similar rate of CSF fungal clearance and 10-week mortality as amphotericin B deoxycholate when combined with flucytosine for the treatment of HIV-associated cryptococcal meningitis.
Trial registration: ClinicalTrials.gov NCT04031833.
Keywords: HIV; amphotericin B deoxycholate; antifungal; cryptococcal meningitis; liposomal amphotericin B.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America. All rights reserved. For commercial re-use, please contact reprints@oup.com for reprints and translation rights for reprints. All other permissions can be obtained through our RightsLink service via the Permissions link on the article page on our site—for further information please contact journals.permissions@oup.com.
Conflict of interest statement
Figures
References
-
- World Health Organization . Guidelines for diagnosing, preventing and managing cryptococcal disease among adults, adolescents and children living with HIV. 2022. . Available at: https://www.who.int/publications/i/item/9789240052178. Accessed 27 June 2022. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- R01 NS110519/NS/NINDS NIH HHS/United States
- R01 NS086312/NS/NINDS NIH HHS/United States
- K23 NS110470/NS/NINDS NIH HHS/United States
- UL1 TR002494/TR/NCATS NIH HHS/United States
- UK Medical Research Council
- TRIA2015-1092/larger AMBITION-cm trial
- KL2 TR002492/TR/NCATS NIH HHS/United States
- European and Developing Countries Clinical Trials Partnership
- KL2TR002492/TR/NCATS NIH HHS/United States
- NH/NIH HHS/United States
- Swedish International Development Cooperation Agency
- D43TW009345/TW/FIC NIH HHS/United States
- MR/P006922/1/Joint Global Health Trials scheme
- WT_/Wellcome Trust/United Kingdom
- D43 TW009345/TW/FIC NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
