

Double contrast-enhanced ultrasonography improves diagnostic accuracy of T staging compared with multi-detector computed tomography in gastric cancer patients
- PMID: 38946876
- PMCID: PMC11212705
- DOI: 10.3748/wjg.v30.i23.3005
Double contrast-enhanced ultrasonography improves diagnostic accuracy of T staging compared with multi-detector computed tomography in gastric cancer patients
Abstract
Background: Gastric cancer (GC) is the most common malignant tumor and ranks third for cancer-related deaths among the worldwide. The disease poses a serious public health problem in China, ranking fifth for incidence and third for mortality. Knowledge of the invasive depth of the tumor is vital to treatment decisions.
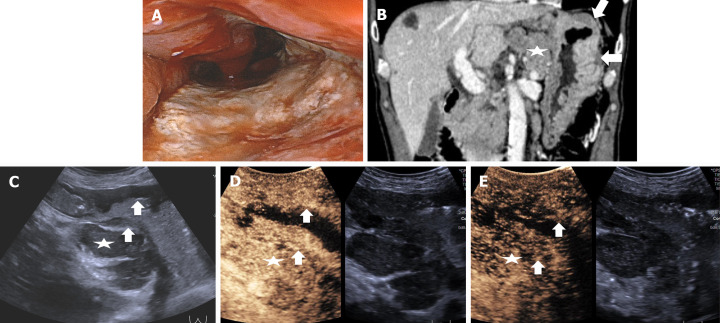
Aim: To evaluate the diagnostic performance of double contrast-enhanced ultrasonography (DCEUS) for preoperative T staging in patients with GC by comparing with multi-detector computed tomography (MDCT).
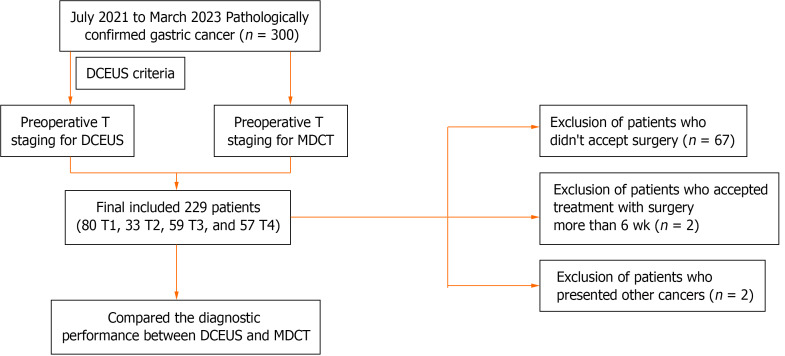
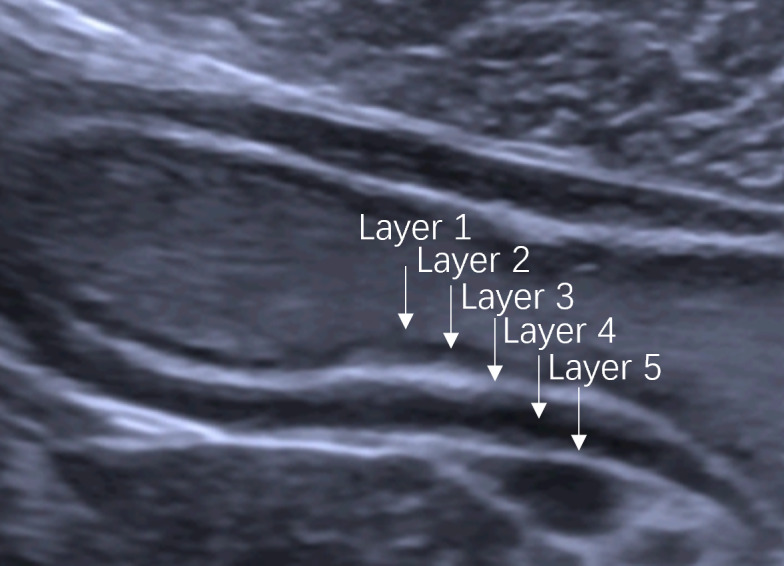
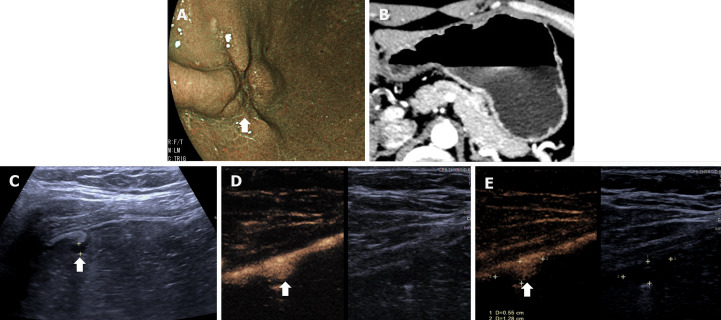
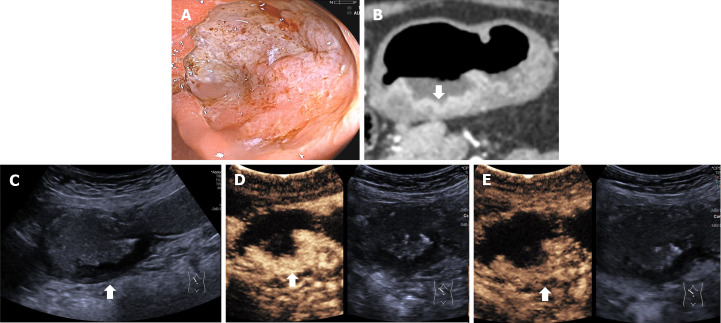
Methods: This single prospective study enrolled patients with GC confirmed by preoperative gastroscopy from July 2021 to March 2023. Patients underwent DCEUS, including ultrasonography (US) and intravenous contrast-enhanced ultrasonography (CEUS), and MDCT examinations for the assessment of preoperative T staging. Features of GC were identified on DCEUS and criteria developed to evaluate T staging according to the 8th edition of AJCC cancer staging manual. The diagnostic performance of DCEUS was evaluated by comparing it with that of MDCT and surgical-pathological findings were considered as the gold standard.
Results: A total of 229 patients with GC (80 T1, 33 T2, 59 T3 and 57 T4) were included. Overall accuracies were 86.9% for DCEUS and 61.1% for MDCT (P < 0.001). DCEUS was superior to MDCT for T1 (92.5% vs 70.0%, P < 0.001), T2 (72.7% vs 51.5%, P = 0.041), T3 (86.4% vs 45.8%, P < 0.001) and T4 (87.7% vs 70.2%, P = 0.022) staging of GC.
Conclusion: DCEUS improved the diagnostic accuracy of preoperative T staging in patients with GC compared with MDCT, and constitutes a promising imaging modality for preoperative evaluation of GC to aid individualized treatment decision-making.
Keywords: Double contrast-enhanced ultrasonography; Gastric cancer; Multi-detector computed tomography; T staging.
©The Author(s) 2024. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All authors declare that they have no conflict of interest.
Figures

Similar articles
-
Preoperative T staging of advanced gastric cancer using double contrast-enhanced ultrasound.Ultraschall Med. 2012 Dec;33(7):E218-E224. doi: 10.1055/s-0032-1312958. Epub 2012 Jun 28. Ultraschall Med. 2012. PMID: 22744445
-
Preoperative Gross Classification of Gastric Adenocarcinoma: Comparison of Double Contrast-Enhanced Ultrasound and Multi-Detector Row CT.Ultrasound Med Biol. 2016 Jul;42(7):1431-40. doi: 10.1016/j.ultrasmedbio.2016.01.030. Epub 2016 Apr 9. Ultrasound Med Biol. 2016. PMID: 27072076
-
Double contrast-enhanced ultrasound for the preoperative gross classification of gastric cancer: a comparison with multidetector computed tomography.BMC Med Imaging. 2022 Dec 21;22(1):223. doi: 10.1186/s12880-022-00954-8. BMC Med Imaging. 2022. PMID: 36544108 Free PMC article.
-
Diagnostic Accuracy of Double Contrast-Enhanced Ultrasonography in Clarifying Tumor Depth (T Stage) of Gastric Cancer: Meta-analysis.Ultrasound Med Biol. 2021 Sep;47(9):2483-2493. doi: 10.1016/j.ultrasmedbio.2021.05.017. Epub 2021 Jun 23. Ultrasound Med Biol. 2021. PMID: 34172338 Review.
-
Updated Evaluation of the Diagnostic Performance of Double Contrast-Enhanced Ultrasonography in the Preoperative T Staging of Gastric Cancer: A Meta-Analysis and Systematic Review.Front Oncol. 2022 Mar 9;12:844390. doi: 10.3389/fonc.2022.844390. eCollection 2022. Front Oncol. 2022. PMID: 35356215 Free PMC article.
References
-
- Ajani JA, D'Amico TA, Bentrem DJ, Chao J, Cooke D, Corvera C, Das P, Enzinger PC, Enzler T, Fanta P, Farjah F, Gerdes H, Gibson MK, Hochwald S, Hofstetter WL, Ilson DH, Keswani RN, Kim S, Kleinberg LR, Klempner SJ, Lacy J, Ly QP, Matkowskyj KA, McNamara M, Mulcahy MF, Outlaw D, Park H, Perry KA, Pimiento J, Poultsides GA, Reznik S, Roses RE, Strong VE, Su S, Wang HL, Wiesner G, Willett CG, Yakoub D, Yoon H, McMillian N, Pluchino LA. Gastric Cancer, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2022;20:167–192. - PubMed
-
- Zheng RS, Chen R, Han BF, Wang SM, Li L, Sun KX, Zeng HM, Wei WW, He J. [Cancer incidence and mortality in China, 2022] Zhonghua Zhong Liu Za Zhi. 2024;46:221–231. - PubMed
-
- Spolverato G, Ejaz A, Kim Y, Squires MH, Poultsides GA, Fields RC, Schmidt C, Weber SM, Votanopoulos K, Maithel SK, Pawlik TM. Use of endoscopic ultrasound in the preoperative staging of gastric cancer: a multi-institutional study of the US gastric cancer collaborative. J Am Coll Surg. 2015;220:48–56. - PubMed
-
- Abdalla EK, Pisters PW. Staging and preoperative evaluation of upper gastrointestinal malignancies. Semin Oncol. 2004;31:513–529. - PubMed
-
- Kwee RM, Kwee TC. Imaging in local staging of gastric cancer: a systematic review. J Clin Oncol. 2007;25:2107–2116. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
