

In vivo modeling recapitulates radiotherapy delivery and late-effect profile for childhood medulloblastoma
- PMID: 38946880
- PMCID: PMC11212071
- DOI: 10.1093/noajnl/vdae091
In vivo modeling recapitulates radiotherapy delivery and late-effect profile for childhood medulloblastoma
Abstract
Background: Medulloblastoma (MB) is the most common malignant pediatric brain tumor, with 5-year survival rates > 70%. Cranial radiotherapy (CRT) to the whole brain, with posterior fossa boost (PFB), underpins treatment for non-infants; however, radiotherapeutic insult to the normal brain has deleterious consequences to neurocognitive and physical functioning, and causes accelerated aging/frailty. Approaches to ameliorate radiotherapy-induced late-effects are lacking and a paucity of appropriate model systems hinders their development.
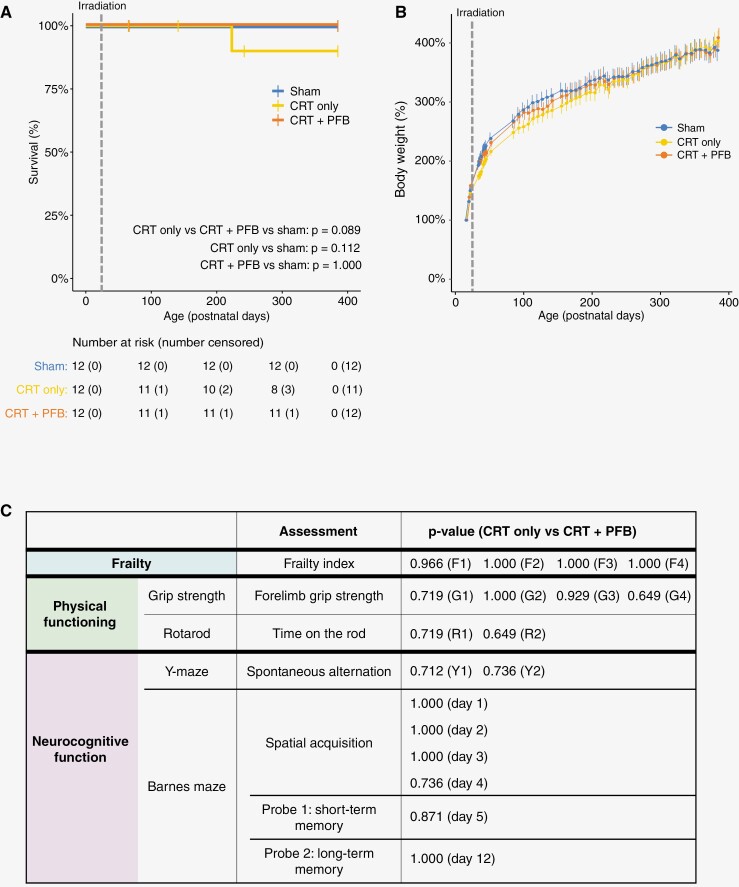
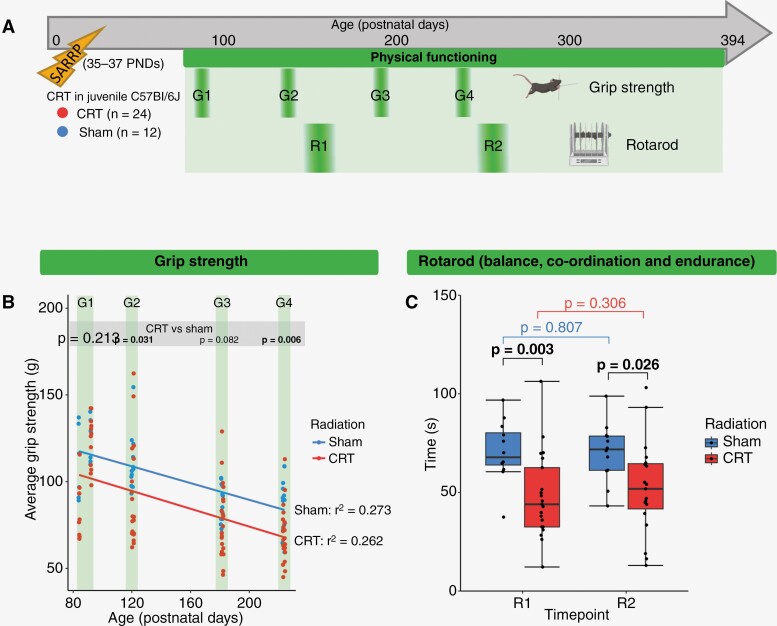
Methods: We have developed a clinically relevant in vivo model system that recapitulates the radiotherapy dose, targeting, and developmental stage of childhood medulloblastoma. Consistent with human regimens, age-equivalent (postnatal days 35-37) male C57Bl/6J mice received computerized tomography image-guided CRT (human-equivalent 37.5 Gy EQD2, n = 12) ± PFB (human-equivalent 48.7 Gy EQD2, n = 12), via the small animal radiation research platform and were longitudinally assessed for > 12 months.
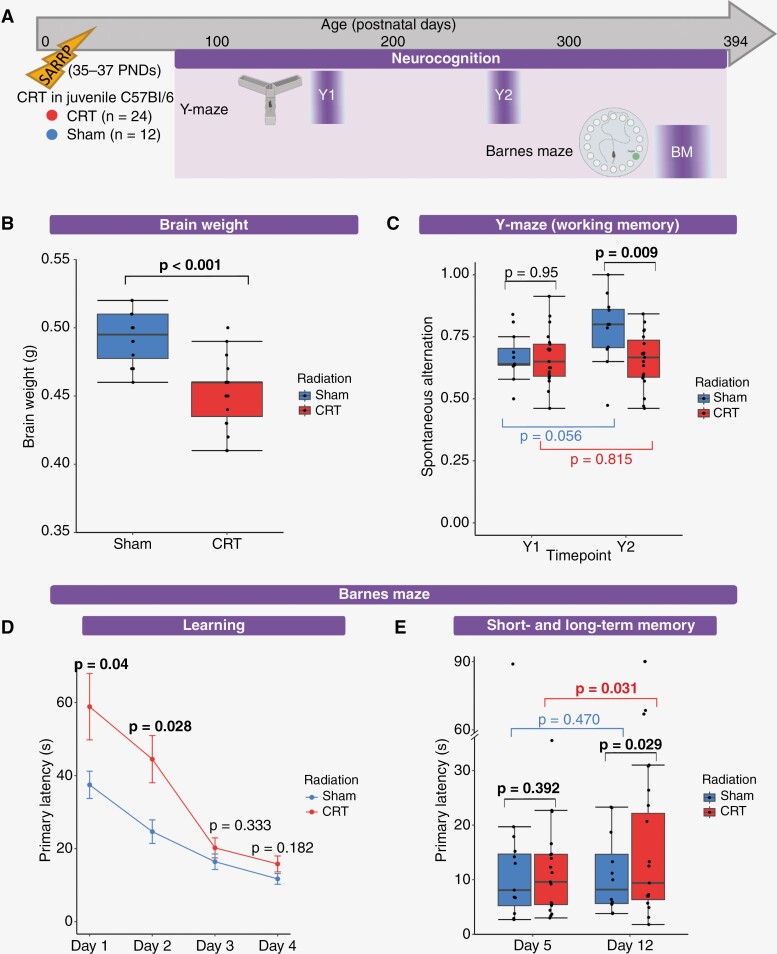
Results: CRT was well tolerated, independent of PFB receipt. Compared to a sham-irradiated group (n = 12), irradiated mice were significantly frailer following irradiation (frailty index; P = .0002) and had reduced physical functioning; time to fall from a rotating rod (rotarod; P = .026) and grip strength (P = .006) were significantly lower. Neurocognitive deficits were consistent with childhood MB survivors; irradiated mice displayed significantly worse working memory (Y-maze; P = .009) and exhibited spatial memory deficits (Barnes maze; P = .029). Receipt of PFB did not induce a more severe late-effect profile.
Conclusions: Our in vivo model mirrored childhood MB radiotherapy and recapitulated features observed in the late-effect profile of MB survivors. Our clinically relevant model will facilitate both the elucidation of novel/target mechanisms underpinning MB late effects and the development of novel interventions for their amelioration.
Keywords: late-effects; medulloblastoma; modelling; radiotherapy; survivorship.
© The Author(s) 2024. Published by Oxford University Press, the Society for Neuro-Oncology and the European Association of Neuro-Oncology.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures


References
-
- Childhood Cancer Statistics. England Annual report 2018. UK: Public Health England.
-
- Oeffinger KC, Mertens AC, Sklar CA, et al. ; Childhood Cancer Survivor Study. Chronic health conditions in adult survivors of childhood cancer. N Engl J Med. 2006;355(15):1572–1582. - PubMed
-
- MacDonald C, Theurer JA, Doyle PC.. “Cured” but not “healed”: The application of principles of palliative care to cancer survivorship. Soc Sci Med. 2021;275(1):113802. - PubMed
-
- Khalil J, Chaabi S, Oberlin O, et al. Medulloblastoma in childhood: What effects on neurocognitive functions? Cancer Radiother. 2019;23(5):370–377. - PubMed
-
- Limond JA, Bull KS, Calaminus G, et al. ; Brain Tumour Quality of Survival Group, International Society of Paediatric Oncology (Europe; SIOP-E). Quality of survival assessment in European childhood brain tumour trials, for children aged 5 years and over. Eur J Paediatr Neurol. 2015;19(2):202–210. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous