

Design and validation of a GMP stem cell manufacturing protocol for MPSII hematopoietic stem cell gene therapy
- PMID: 38946936
- PMCID: PMC11214401
- DOI: 10.1016/j.omtm.2024.101271
Design and validation of a GMP stem cell manufacturing protocol for MPSII hematopoietic stem cell gene therapy
Abstract
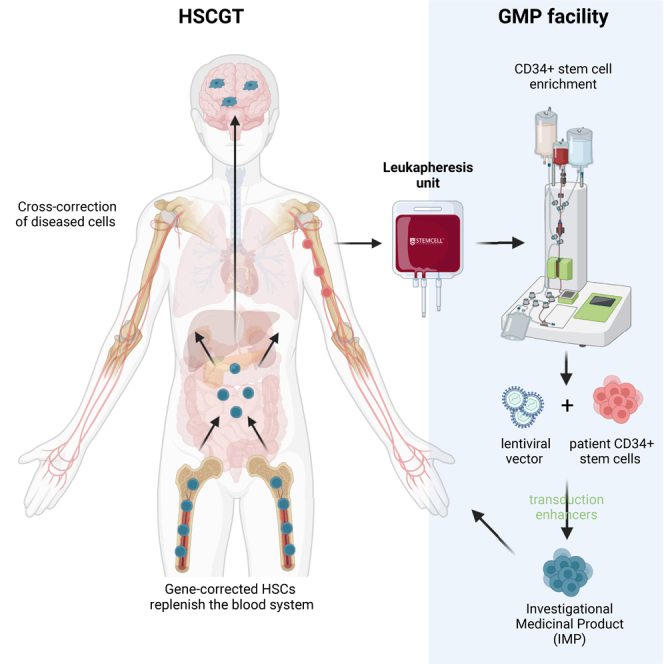
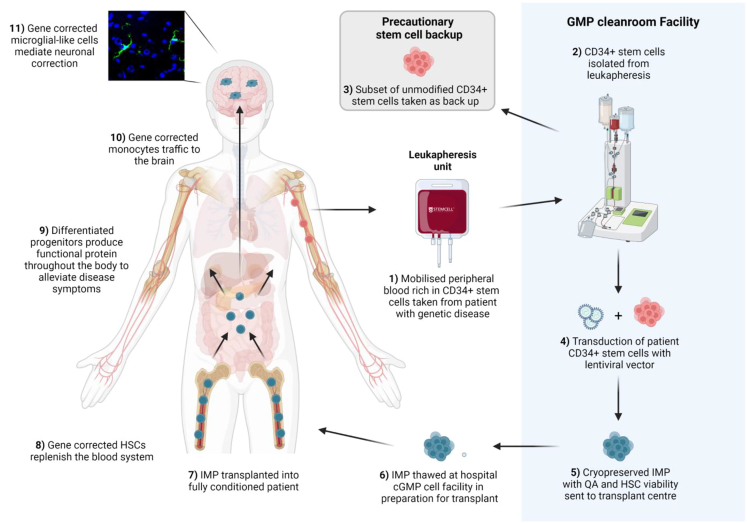
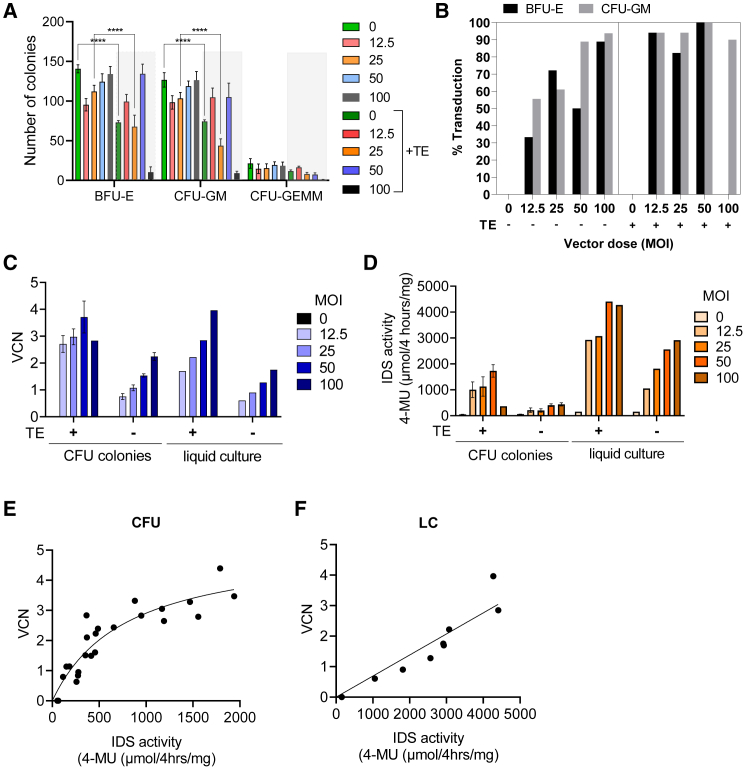
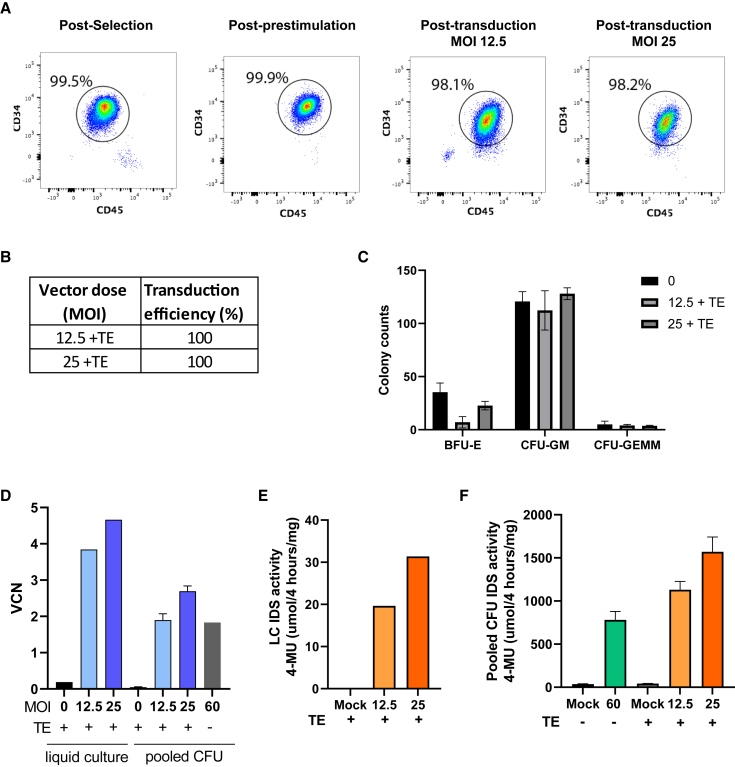
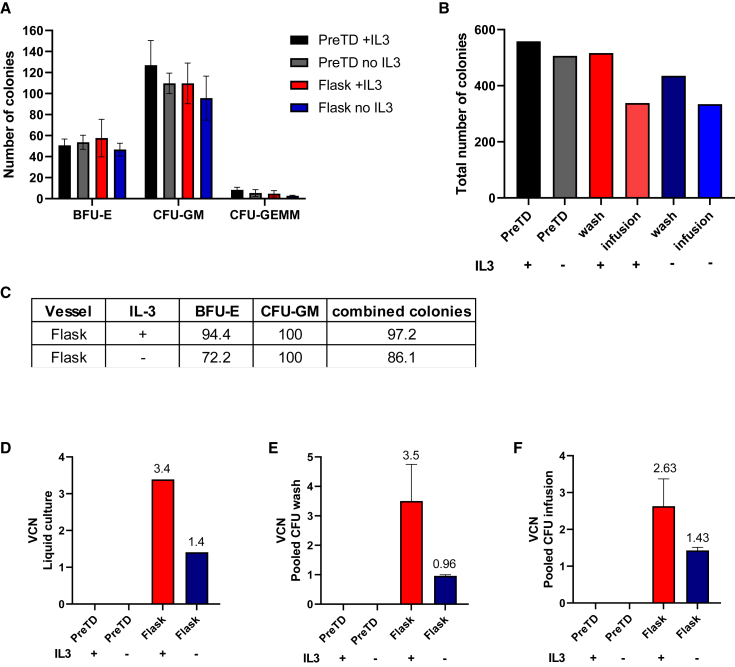
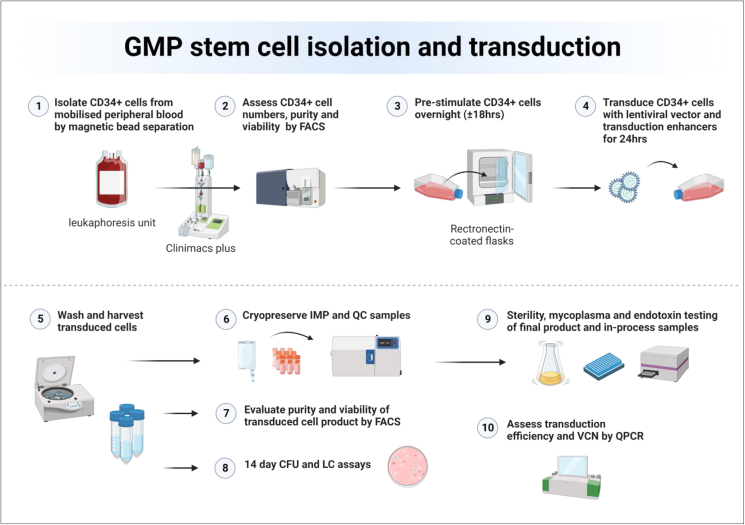
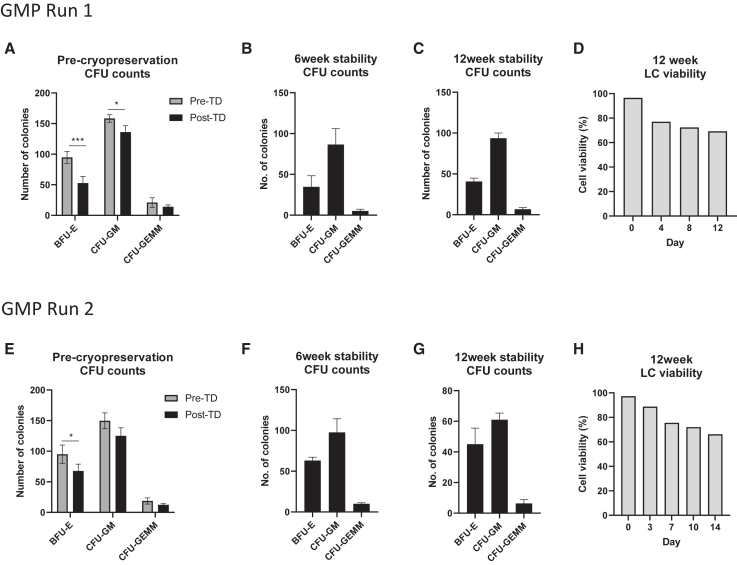
Hematopoietic stem cell gene therapy (HSCGT) is a promising therapeutic strategy for the treatment of neurodegenerative, metabolic disorders. The approach involves the ex vivo introduction of a missing gene into patients' own stem cells via lentiviral-mediated transduction (TD). Once transplanted back into a fully conditioned patient, these genetically modified HSCs can repopulate the blood system and produce the functional protein, previously absent or non-functional in the patient, which can then cross-correct other affected cells in somatic organs and the central nervous system. We previously developed an HSCGT approach for the treatment of Mucopolysaccharidosis type II (MPSII) (Hunter syndrome), a debilitating pediatric lysosomal disorder caused by mutations in the iduronate-2-sulphatase (IDS) gene, leading to the accumulation of heparan and dermatan sulfate, which causes severe neurodegeneration, skeletal abnormalities, and cardiorespiratory disease. In HSCGT proof-of-concept studies using lentiviral IDS fused to a brain-targeting peptide ApoEII (IDS.ApoEII), we were able to normalize brain pathology and behavior of MPSII mice. Here we present an optimized and validated good manufacturing practice hematopoietic stem cell TD protocol for MPSII in preparation for first-in-man studies. Inclusion of TEs LentiBOOST and protamine sulfate significantly improved TD efficiency by at least 3-fold without causing adverse toxicity, thereby reducing vector quantity required.
Keywords: GMP cell manufacturing; MPSII; cleanroom validation studies; hCD34+ cell transduction; hematopoietic stem cell gene therapy; investigational medicinal product; lentiviral vector; mucopolysaccharidosis; transduction enhancers.
© 2024 The Authors.
Conflict of interest statement
B.W.B. holds a patent for the use of the IDS.ApoEII in the treatment of MPSII and is the recipient of a clinical trial grant from AVROBIO for the treatment of MPSII with LV.IDS.ApoEII.
Figures
Similar articles
-
Sustained long-term disease correction in a murine model of MPSII following stem cell gene therapy.Mol Ther Methods Clin Dev. 2023 Oct 20;31:101127. doi: 10.1016/j.omtm.2023.101127. eCollection 2023 Dec 14. Mol Ther Methods Clin Dev. 2023. PMID: 37920237 Free PMC article.
-
Establishment of the Effectiveness of Early Versus Late Stem Cell Gene Therapy in Mucopolysaccharidosis II for Treating Central Versus Peripheral Disease.Hum Gene Ther. 2024 Apr;35(7-8):243-255. doi: 10.1089/hum.2023.002. Epub 2023 Aug 30. Hum Gene Ther. 2024. PMID: 37427450
-
Fusion of Rabies Virus Glycoprotein or gh625 to Iduronate-2-Sulfatase for the Treatment of Mucopolysaccharidosis Type II.Hum Gene Ther. 2024 Apr;35(7-8):232-242. doi: 10.1089/hum.2023.025. Epub 2023 Jul 7. Hum Gene Ther. 2024. PMID: 37212263
-
Gene Therapy for Mucopolysaccharidosis Type II-A Review of the Current Possibilities.Int J Mol Sci. 2021 May 23;22(11):5490. doi: 10.3390/ijms22115490. Int J Mol Sci. 2021. PMID: 34070997 Free PMC article. Review.
-
Hematopoietic Stem Cell Gene Therapy for Cystinosis: From Bench-to-Bedside.Cells. 2021 Nov 23;10(12):3273. doi: 10.3390/cells10123273. Cells. 2021. PMID: 34943781 Free PMC article. Review.
Cited by
-
Development of a Lentiviral Vector for High-Yield Production of Synthetic and Recombinant GCase for Gaucher Disease Therapy.Int J Mol Sci. 2025 Jul 23;26(15):7089. doi: 10.3390/ijms26157089. Int J Mol Sci. 2025. PMID: 40806226 Free PMC article.
-
Lentiviral Vector-Mediated Ex Vivo Hematopoietic Stem Cell Gene Therapy for Mucopolysaccharidosis IVA Murine Model.Hum Gene Ther. 2024 Nov;35(21-22):917-937. doi: 10.1089/hum.2024.094. Epub 2024 Oct 24. Hum Gene Ther. 2024. PMID: 39446675
-
Human iPSC-derived neural stem cells engraft and improve pathophysiology of MPS I mice.Mol Ther Methods Clin Dev. 2024 Nov 5;32(4):101367. doi: 10.1016/j.omtm.2024.101367. eCollection 2024 Dec 12. Mol Ther Methods Clin Dev. 2024. PMID: 39764351 Free PMC article.
References
-
- Fumagalli F., Calbi V., Natali Sora M.G., Sessa M., Baldoli C., Rancoita P.M.V., Ciotti F., Sarzana M., Fraschini M., Zambon A.A., et al. Lentiviral haematopoietic stem-cell gene therapy for early-onset metachromatic leukodystrophy: long-term results from a non-randomised, open-label, phase 1/2 trial and expanded access. Lancet. 2022;399:372–383. doi: 10.1016/S0140-6736(21)02017-1. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
