

This is a preprint.
JAK inhibition decreases the autoimmune burden in Down syndrome
- PMID: 38946973
- PMCID: PMC11213071
- DOI: 10.1101/2024.06.13.24308783
JAK inhibition decreases the autoimmune burden in Down syndrome
Update in
-
JAK inhibition decreases the autoimmune burden in Down syndrome.Elife. 2024 Dec 31;13:RP99323. doi: 10.7554/eLife.99323. Elife. 2024. PMID: 39737640 Free PMC article. Clinical Trial.
Abstract
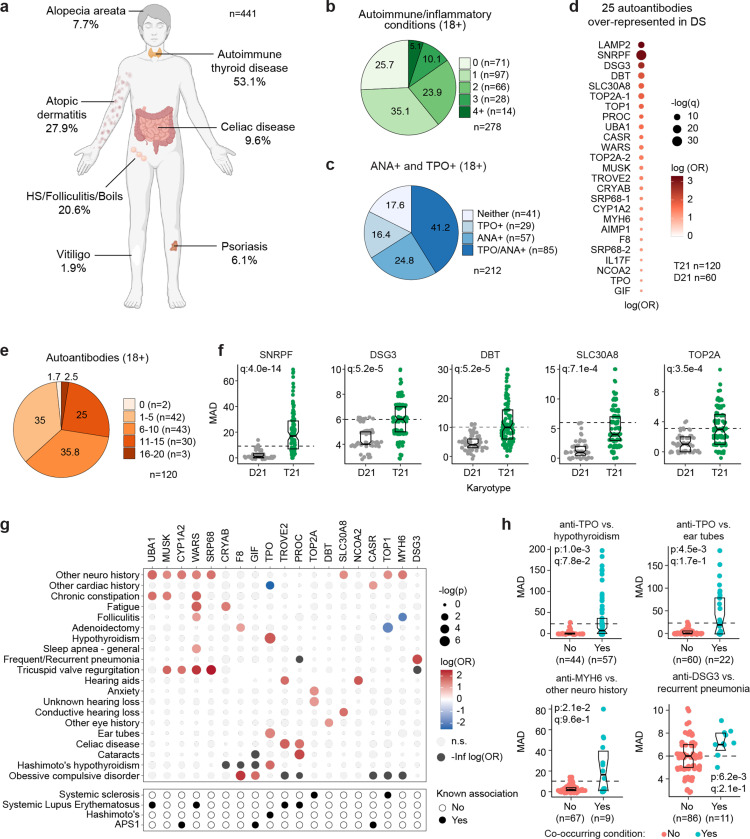
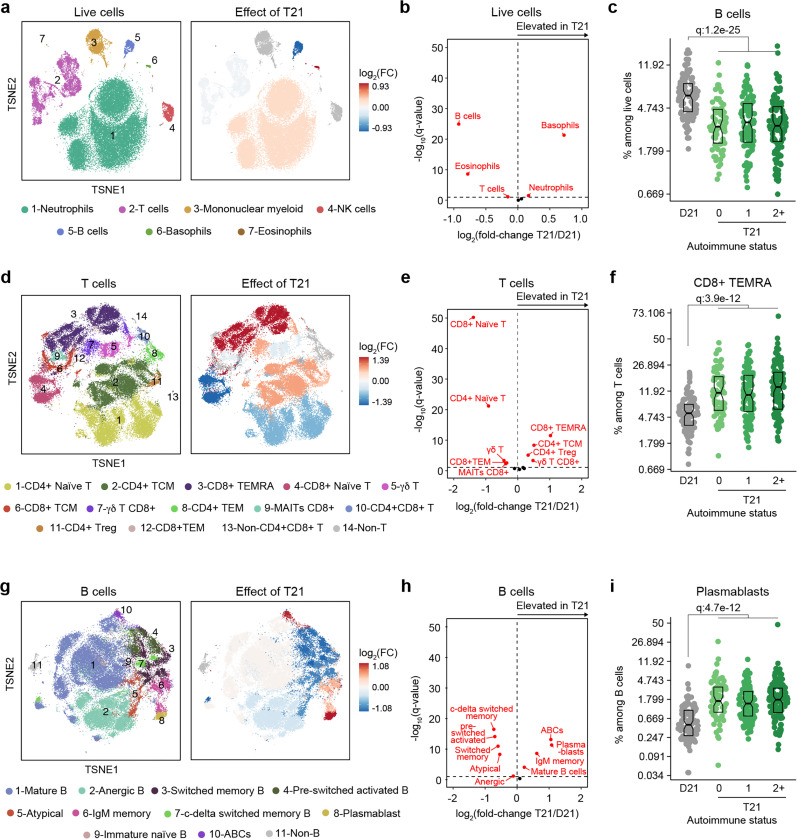
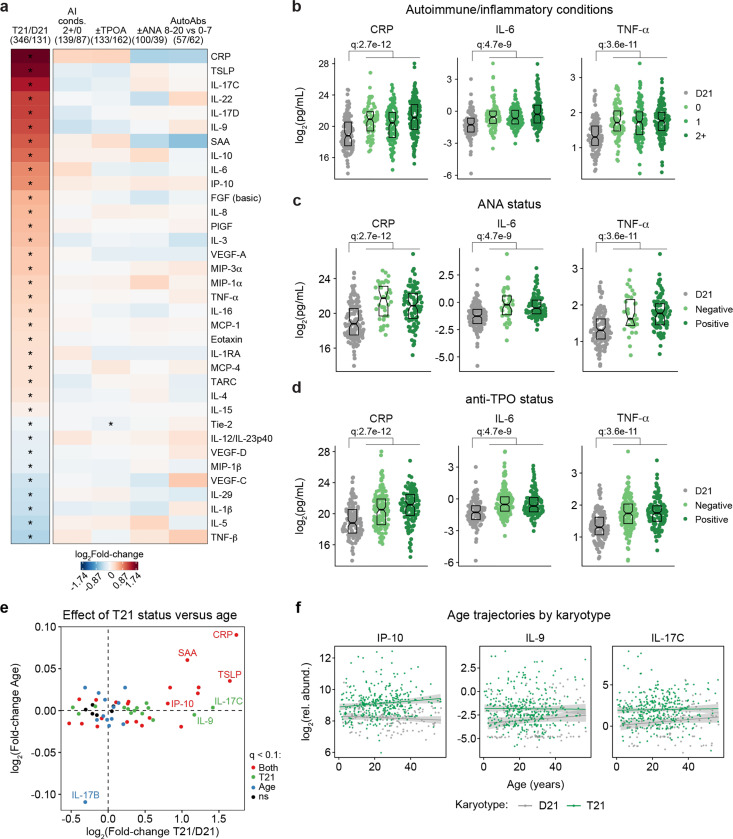
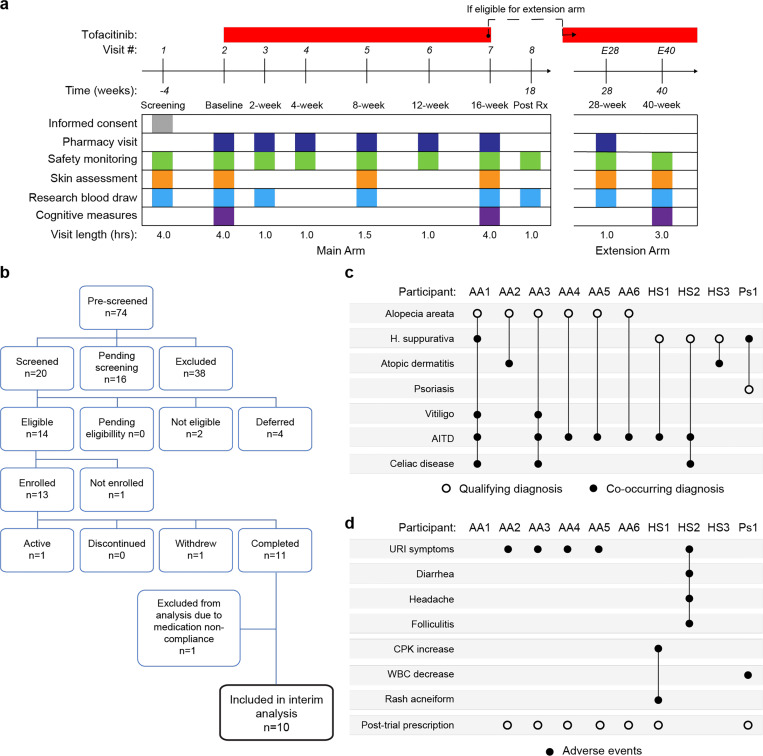
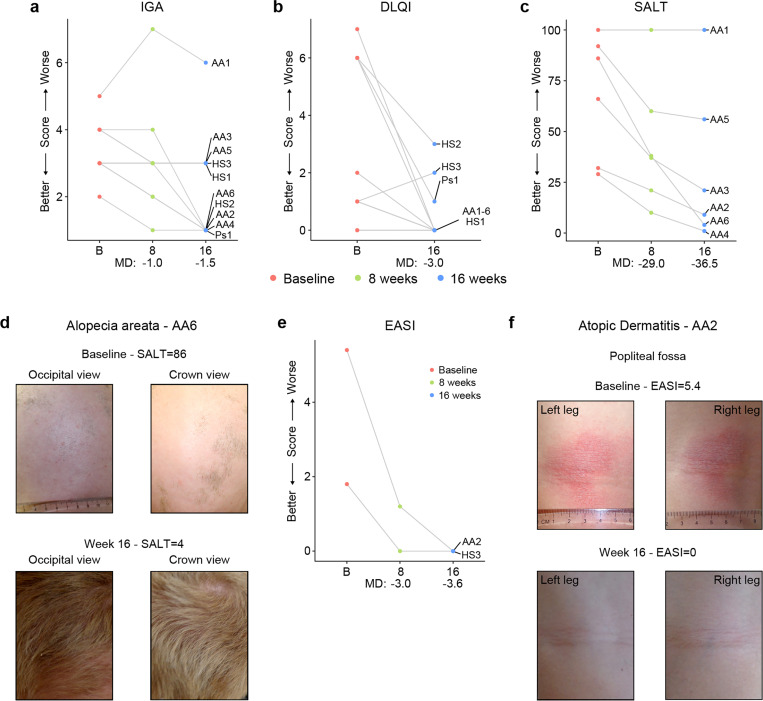
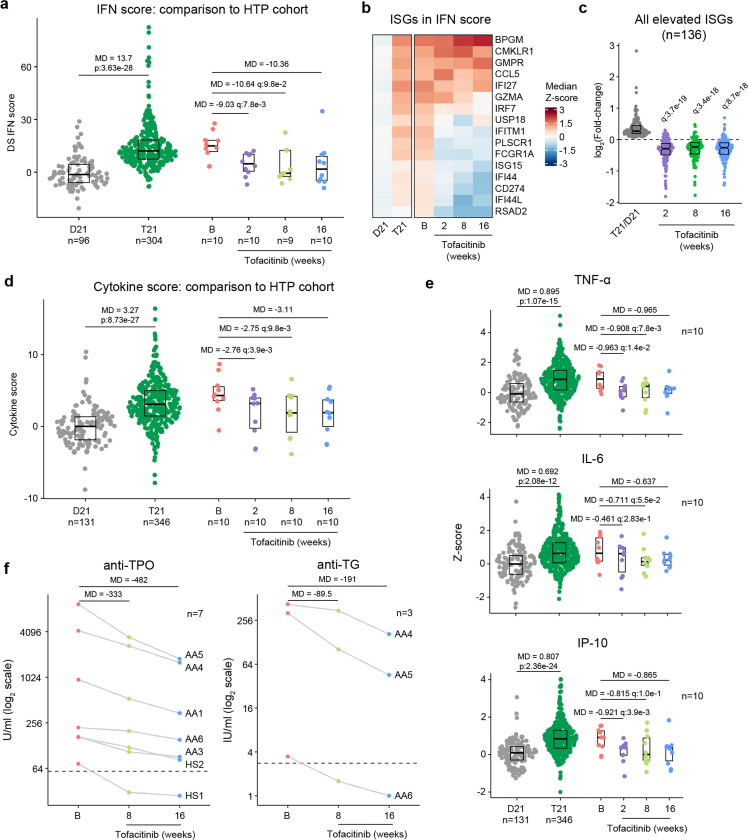
Individuals with Down syndrome (DS), the genetic condition caused by trisomy 21 (T21), display clear signs of immune dysregulation, including high rates of autoimmune disorders and severe complications from infections. Although it is well established that T21 causes increased interferon responses and JAK/STAT signaling, elevated autoantibodies, global immune remodeling, and hypercytokinemia, the interplay between these processes, the clinical manifestations of DS, and potential therapeutic interventions remain ill defined. Here, we report a comprehensive analysis of immune dysregulation at the clinical, cellular, and molecular level in hundreds of individuals with DS. We demonstrate multi-organ autoimmunity of pediatric onset concurrent with unexpected autoantibody-phenotype associations. Importantly, constitutive immune remodeling and hypercytokinemia occur from an early age prior to autoimmune diagnoses or autoantibody production. We then report the interim analysis of a Phase II clinical trial investigating the safety and efficacy of the JAK inhibitor tofacitinib through multiple clinical and molecular endpoints. Analysis of the first 10 participants to complete the 16-week study shows a good safety profile and no serious adverse events. Treatment reduced skin pathology in alopecia areata, psoriasis, and atopic dermatitis, while decreasing interferon scores, cytokine scores, and levels of pathogenic autoantibodies without overt immune suppression. Additional research is needed to define the effects of JAK inhibition on the broader developmental and clinical hallmarks of DS. ClinicalTrials.gov identifier: NCT04246372.
Conflict of interest statement
Competing Interests Statement: J.M.E. has provided consulting services for Eli Lilly Co., Gilead Sciences Inc., and Biohaven Pharmaceuticals and serves on the advisory board of Perha Pharmaceuticals. The remaining authors declare no competing interests.
Figures
References
-
- Lejeune J., Turpin R. & Gautier M. [Mongolism; a chromosomal disease (trisomy)]. Bull Acad Natl Med 143, 256–265 (1959). - PubMed
Publication types
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases