

This is a preprint.
Germline prediction of immune checkpoint inhibitor discontinuation for immune-related adverse events
- PMID: 38947092
- PMCID: PMC11213033
- DOI: 10.1101/2024.06.10.24308518
Germline prediction of immune checkpoint inhibitor discontinuation for immune-related adverse events
Update in
-
Germline prediction of immune checkpoint inhibitor discontinuation for immune-related adverse events.J Immunother Cancer. 2025 Mar 28;13(3):e011273. doi: 10.1136/jitc-2024-011273. J Immunother Cancer. 2025. PMID: 40154961 Free PMC article.
Abstract
Introduction: Immune checkpoint inhibitors (ICIs) can yield remarkable clinical responses in subsets of patients with solid tumors but can also often lead to immune-related adverse events (irAEs). Predictive features of clinically severe irAEs leading to cessation of ICIs have yet to be established. Using data from 1,327 patients with lung cancer treated with ICIs between 2009 and 2022 at four academic medical centers, we evaluated the association of a germline polygenic risk score for autoimmune disease and discontinuation of ICIs due to irAEs.
Methods: Using Cox proportional hazards model, we assessed the association between a polygenic risk score for autoimmune disease (PRSAD) and cessation of ICI therapy due to irAEs. All models were adjusted for age at diagnosis, sex, lung cancer histology, type of therapy, recruiting center, and the first 5 principal components. To further understand the differential effects of type of therapy and disease stage on the association between PRSAD and cessation of ICI due to irAEs, we conducted stratified logistic regression analysis by type of ICI therapy and disease stage.
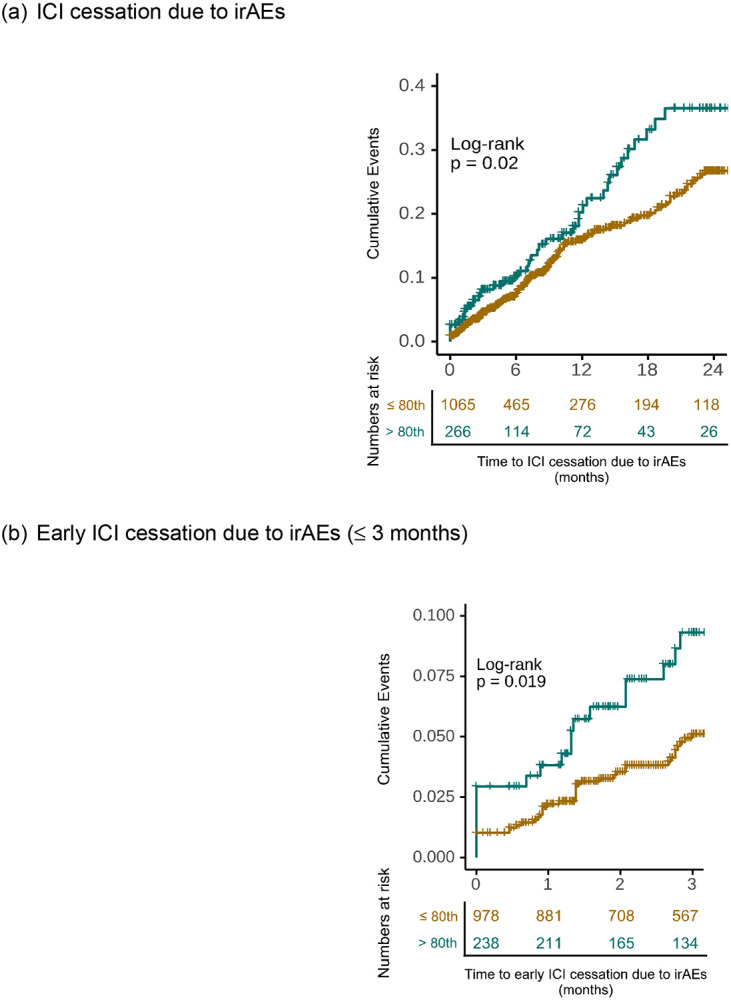
Results: We found an association between PRSAD and ICI cessation due to irAEs (HR per SD = 1.18, 95% CI = 1.02 - 1.37, P = 0.03). This association was particularly strong in patients who had ICI cessation due to irAEs within three months of therapy initiation (HR per SD = 1.38, 95% CI = 1.08 - 1.78, P = 0.01). Individuals in the top 20th percentile of PRSAD had 7.2% ICI discontinuation for irAEs by three months, compared to 3.9% discontinuation by three months among patients in the bottom 80th percentile (log-rank P = 0.02). In addition, among patients who received combination PD-1/PD-L1 and CTLA-4 inhibitor therapy, PRSAD had an OR per SD of 1.86 (95% CI = 1.08 - 3.51, P = 0.04).
Conclusions: We demonstrate an association between a polygenic risk score for autoimmune disease and early ICI discontinuation for irAEs, particularly among patients treated with combination ICI therapy. Our results suggest that germline genetics may be used as an adjunctive tool for risk stratification around ICI clinical decision-making in solid tumor oncology.
Figures


References
-
- Wei SC, Duffy CR, Allison JP. Fundamental Mechanisms of Immune Checkpoint Blockade Therapy. Cancer Discovery. 2018;8(9):1069–1086. doi: 10.1158/2159-8290.CD-18-0367 - DOI - PubMed
Publication types
Grants and funding
- S10 OD017985/OD/NIH HHS/United States
- UL1 TR000445/TR/NCATS NIH HHS/United States
- R01 CA227466/CA/NCI NIH HHS/United States
- T32 CA009207/CA/NCI NIH HHS/United States
- U19 HL065962/HL/NHLBI NIH HHS/United States
- S10 RR025141/RR/NCRR NIH HHS/United States
- R01 CA251758/CA/NCI NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- UG1 CA233259/CA/NCI NIH HHS/United States
- R01 HD074711/HD/NICHD NIH HHS/United States
- RC2 GM092618/GM/NIGMS NIH HHS/United States
- P30 CA068485/CA/NCI NIH HHS/United States
- U01 HG006378/HG/NHGRI NIH HHS/United States
- K24 CA169004/CA/NCI NIH HHS/United States
- P01 CA129243/CA/NCI NIH HHS/United States
- U01 CA253560/CA/NCI NIH HHS/United States
- K12 DK133995/DK/NIDDK NIH HHS/United States
- P50 GM115305/GM/NIGMS NIH HHS/United States
- UL1 RR024975/RR/NCRR NIH HHS/United States
- R01 NS032830/NS/NINDS NIH HHS/United States
- U01 HG004798/HG/NHGRI NIH HHS/United States
- UL1 TR002243/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Research Materials