

Cardiotoxicity of CPX-351 in children and adolescents with relapsed AML: a Children's Oncology Group report
- PMID: 38947228
- PMCID: PMC11211570
- DOI: 10.3389/fcvm.2024.1347547
Cardiotoxicity of CPX-351 in children and adolescents with relapsed AML: a Children's Oncology Group report
Abstract
Introduction: Anthracyclines are effective in treating acute myeloid leukemia (AML) but limited by cardiotoxicity. CPX-351, a liposomal daunorubicin and cytarabine, may provide therapeutic benefit with less cardiotoxicity. Acute changes in left ventricular systolic function and cardiac biomarkers were evaluated after a cycle of CPX-351 in children with relapsed AML treated on the phase 1/2 Children's Oncology Group study, AAML1421.
Methods: Subjects received 135 units/m2/dose of CPX-351 on days 1, 3, and 5 as cycle 1. Echocardiograms were performed and centrally quantitated at baseline and at the end of cycle 1 (day 29 +/- 1 week). High sensitivity troponin (hs-cTnT) and N-terminal pro-B-type natriuretic peptide (NT-proBNP) were measured at baseline and serially through the end of cycle 1 (days 5, 8, 15, 22 and 29). Differences between baseline and post-CPX-351 echo/biomarker measures were analyzed using Wilcoxon signed rank tests. Linear regression was used to model post-CPX-351 left ventricular ejection fraction (LVEF) with cTnT/NT-proBNP at each time point, controlling for baseline LVEF. Cancer therapy related cardiac dysfunction (CTRCD) was defined as a decline in LVEF of ≥10%-<50%.
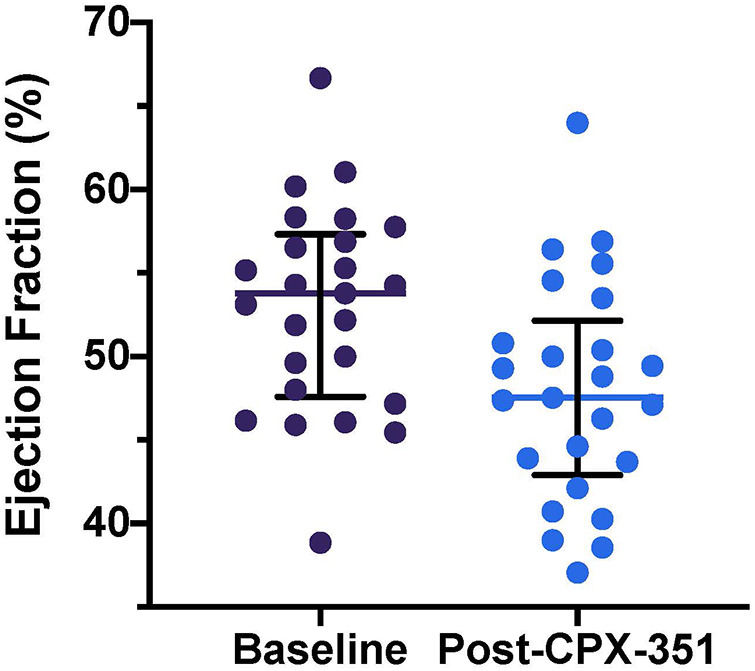
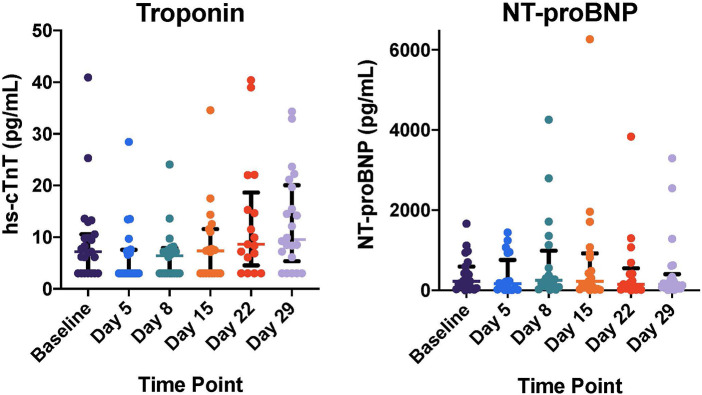
Results: Twenty-five of 38 heavily anthracycline pre-treated (median 348 mg/m2 daunorubicin equivalents) subjects enrolled on AAML1421 were included in the cardiac analyses. At baseline, centrally quantitated LVEF was <50% in 8 of 25 subjects (32%) with a median LVEF of 53.8% [48.0, 56.9]. Following CPX-351, LVEF declined significantly (ΔLVEF -3.3% [-7.8, 0]) and 6 of 25 subjects (24%) experienced CTRCD. Amongst all subjects, hs-cTnT was modestly increased at end of cycle 1 compared to baseline [baseline hs-cTnT 7.2 (3, 10.6); ΔcTnT 1.80 (0, 6.1), p = 0.03]. NT-proBNP remained stably elevated without significant change. No significant associations were seen between NT-proBNP or cTnT levels and post-CPX-351 LVEF.
Discussion: In this single arm study of anthracycline pre-treated children exposed to CPX-351, baseline abnormalities in cardiovascular function were prevalent. Following CPX-351, LVEF decreased, cTnT increased, and NT-proBNP did not change. Longer follow-up is needed to determine whether these changes result in clinically meaningful long-term decrements in cardiac function. An ongoing randomized trial of CPX-351 compared to standard anthracyclines in anthracycline naïve patients will provide further insight into the cardiac effects of CPX-351 (ClinicalTrials.gov; NCT04293562).
Keywords: AAML1421; CPX-351; cardiac biomarkers; cardiotoxicity; liposomal anthracycline; pediatric acute myeloid leukemia (AML); relapse.
© 2024 Leger, Absalon, Demissei, Smith, Gerbing, Alonzo, Narayan, Hirsch, Pollard, Razzouk, Getz, Aplenc, Kolb, Ky and Cooper.
Conflict of interest statement
KL declares: Jazz pharmaceuticals (consulting, advisory board participation); moderate conflict (annual payments $6 k); Abbott Diagnostics (research funding). The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The authors declare that the clinical trial within which these cardiac studies were conducted received drug supply and funding from Jazz Pharmaceuticals. The funder was involved in the review and approval of the clinical trial protocol.
Figures
References
-
- Getz KD, Sung L, Alonzo TA, Leger KJ, Gerbing RB, Pollard JA, et al. Effect of dexrazoxane on left ventricular systolic function and treatment outcomes in patients with acute myeloid leukemia: a report from the children’s oncology group. J Clin Oncol. (2020) 38(21):2398–406. 10.1200/JCO.19.02856 - DOI - PMC - PubMed
-
- Mitchell J, Pfeiffer M, Boehmer J, Gorcsan J, Dronamraju N, Faderl S, et al. Cardiotoxicity of CPX-351 vs 7 + 3 in patients with untreated high-risk acute myeloid leukemia. J Clin Oncol. (2023) 41(16_suppl):7029. 10.1200/JCO.2023.41.16_suppl.7029 - DOI
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials