

Inferior Laryngeal Nerve Paraganglioma With Norepinephrine Hypersecretion Diagnosed Shortly After Pregnancy
- PMID: 38947415
- PMCID: PMC11211820
- DOI: 10.1210/jcemcr/luae107
Inferior Laryngeal Nerve Paraganglioma With Norepinephrine Hypersecretion Diagnosed Shortly After Pregnancy
Abstract
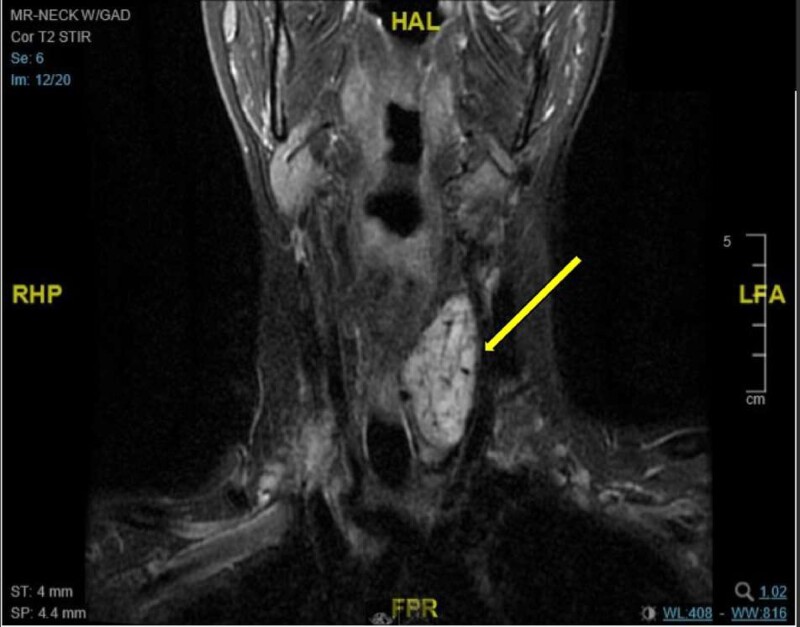
The diagnosis of pheochromocytoma or paraganglioma (PGL) during pregnancy is extremely rare, with 2 large case series suggesting that the prevalence is between 0.0002% and 0.007%. Here, we present a case of a 38-year-old woman who presented during pregnancy with clinical features suggestive of preeclampsia and was found to have a norepinephrine-secreting inferior laryngeal nerve PGL, which was diagnosed after pregnancy. She underwent uncomplicated surgical resection and genetic testing revealed a succinate dehydrogenase subunit B (SDHB) pathogenic variant. In conclusion, PGLs diagnosed during pregnancy and hypersecreting head and neck PGLs are both rare clinical entities. Hyperfunctioning PGLs may mimic pregnancy-induced hypertension or preeclampsia. Metanephrine testing should be considered in patients with atypical features and can be reliably assessed using nonpregnant reference ranges. Overall, maternal and fetal mortality has improved considerably with early diagnosis and treatment.
Keywords: laryngeal nerve; norepinephrine; paraganglioma; pregnancy.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Endocrine Society.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous