

A2/A2B Deceased Donor Kidney Transplantation Using A2 Titers Improves Access to Kidney Transplantation: A Single-Center Study
- PMID: 38947773
- PMCID: PMC11214338
- DOI: 10.1016/j.xkme.2024.100843
A2/A2B Deceased Donor Kidney Transplantation Using A2 Titers Improves Access to Kidney Transplantation: A Single-Center Study
Abstract
Rationale & objective: The option for A2/A2B deceased donor kidney transplantation was integrated into the kidney allocation system in 2014 to improve access for B blood group waitlist candidates. Despite excellent reported outcomes, center uptake has remained low across the United States. Here, we examined the effect of implementing an A2/A2B protocol using a cutoff titer of ≤1:8 for IgG and ≤1:16 for IgM on blood group B kidney transplant recipients at a single center.
Study design: Retrospective observational study.
Setting & participants: Blood group B recipients of deceased donor kidney transplants at a single center from January 1, 2019, to December 2022.
Exposure: Recipients of deceased donor kidney transplants were analyzed based on donor blood type with comparisons of A2/A2B versus blood group compatible.
Outcomes: One-year patient survival, death-censored allograft function, primary nonfunction, delayed graft function, allograft function as measured using serum creatinine levels and estimated glomerular filtration rate at 1 year, biopsy-proven rejection, and need for plasmapheresis.
Analytical approach: Comparison between the A2/A2B and compatible groups were performed using the Fisher test or the χ2 test for categorical variables and the nonparametric Wilcoxon rank-sum test for continuous variables.
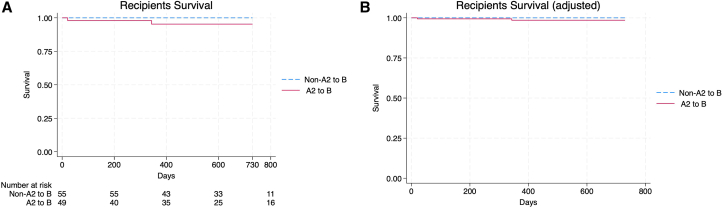
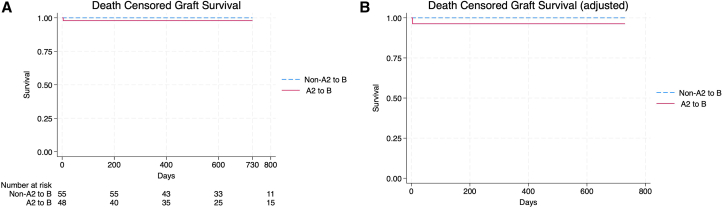
Results: A total of 104 blood type B patients received a deceased donor kidney transplant at our center during the study period, 49 (47.1%) of whom received an A2/A2B transplant. Waiting time was lower in A2/A2B recipients compared with blood group compatible recipients (57.9 months vs 74.7 months, P = 0.01). A2/A2B recipients were more likely to receive a donor after cardiac death (24.5% vs 1.8%, P < 0.05) and experience delayed graft function (65.3% vs 41.8%). There were no observed differences in the average serum creatinine level or estimated glomerular filtration rate at 1 month, 3 months, and 1 year post kidney transplantation, acute rejection, or primary nonfunction.
Limitations: Single-center study. Small cohort size limiting outcome analysis.
Conclusions: Implementation of an A2/A2B protocol increased transplant volumes of blood group B waitlisted patients by 83.6% and decreased the waiting time for transplantation by 22.5% with similar transplant outcomes.
Keywords: ABO incompatible; TK; deceased donor; kidney transplant.
Plain language summary
Recipient blood type is one of the main determinants of waiting time to receive a deceased donor kidney transplant. Patients with blood type B have some of the longest waiting times for a kidney in the United States. Minorities comprise a large percentage of blood group B waitlist patients, contributing to observed racial differences in kidney transplantation rates. In this study, accepting an A2/A2B incompatible kidney resulted in receiving a kidney transplant almost 18 months earlier compared with receiving a blood group compatible kidney. No differences in outcomes were seen by accepting A2/A2B kidneys.
© 2024 The Authors.
Figures
References
-
- Stegall M.D., Dean P.G., Gloor J.M. ABO-incompatible kidney transplantation. Transplantation. 2004;78(5):635–641. - PubMed
-
- Bryan C.F., Cherikh W.S., Sesok-Pizzini D.A. A2/A2B to B renal transplantation: past, present, and future directions. Am J Transplant. 2016;16(1):11–20. - PubMed
-
- Mahapatra S., Mishra D., Sahoo D., Sahoo B.B. Study of prevalence of A2, A2B along with major ABO blood groups to minimize the transfusion reactions. Int J Sci Res. 2016;5(3):189–190.
-
- Breimer M.E., Samuelsson B.E. The specific distribution of glycolipid-based blood group A antigens in human kidney related to A1/A2, Lewis, and secretor status of single individuals. A possible molecular explanation for the successful transplantation of A2 kidneys into O recipients. Transplantation. 1986;42(1):88–91. - PubMed
LinkOut - more resources
Full Text Sources
