

Skeletal muscle injury treatment using the Silk Elastin® injection in a rat model
- PMID: 38948131
- PMCID: PMC11214263
- DOI: 10.1016/j.reth.2024.05.012
Skeletal muscle injury treatment using the Silk Elastin® injection in a rat model
Abstract
Background: Skeletal muscle injury (SMI) is often treated conservatively, although it can lead to scar tissue formation, which impedes muscle function and increases muscle re-injury risk. However, effective interventions for SMIs are yet to be established.
Hypothesis: The administration of Silk Elastin® (SE), a novel artificial protein, to the SMI site can suppress scar formation and promote tissue repair.
Study design: A controlled laboratory study.
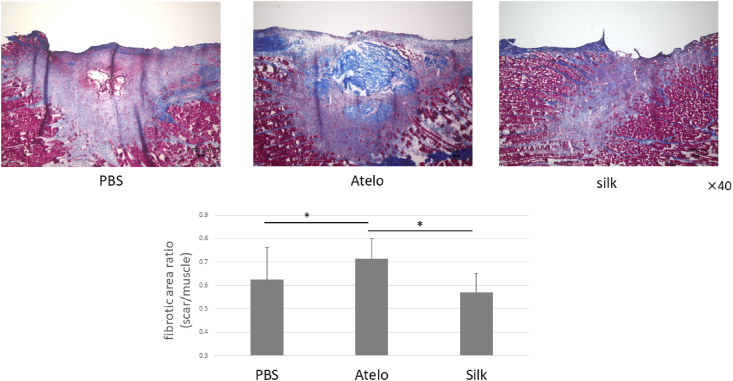
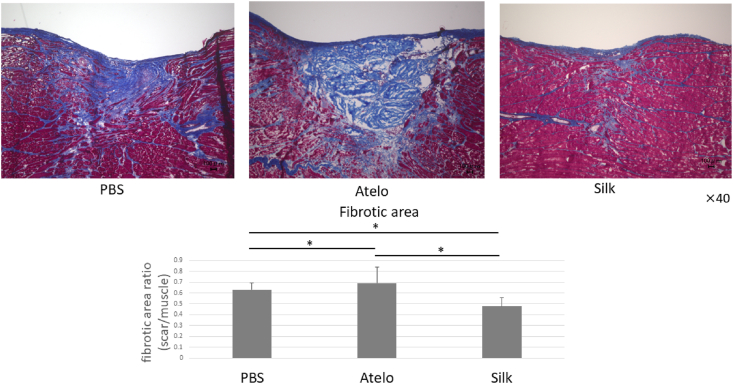
Methods: In vitro: Fibroblast migration ability was assessed using a scratch assay. SE solution was added to the culture medium, and the fibroblast migration ability was compared across different concentrations. In vivo: An SMI model was established with Sprague-Dawley rats, which were assigned to three groups based on the material injected to the SMI site: SE gel (SE group; n = 8), atelocollagen gel (Atelo group; n = 8), and phosphate buffer saline (PBS group; n = 8). Histological evaluations were performed at weeks 1 and 4 following the SMI induction. In the 1-week model, we detected the expression of transforming growth factor (TGF)-β1 in the stroma using immunohistological evaluation and real-time polymerase chain reaction analysis. In the 4-week model, we measured tibialis anterior muscle strength upon peroneal nerve stimulation as a functional assessment.
Results: In vitro: The fibroblast migration ability was suppressed by SE added at a concentration of 10⁴ μg/mL in the culture medium. In vivo: In the 1-week model, the SE group exhibited significantly lower TGFβ -1 expression than the PBS group. In the 4-week model, the SE group had a significantly larger regenerated muscle fiber diameter and smaller scar formation area ratio than the other two groups. Moreover, the SE group was superior to the other two groups in terms of regenerative muscle strength.
Conclusion: Injection of SE gel to the SMI site may inhibit tissue scarring by reducing excessive fibroblast migration, thereby enhancing tissue repair.
Clinical relevance: The findings of this study may contribute to the development of an early intervention method for SMIs.
Keywords: Fibrosis; Injury; Material; Skeletal muscle.
© 2024 The Japanese Society for Regenerative Medicine. Production and hosting by Elsevier B.V.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Kyohei Nakata reports equipment, drugs, or supplies was provided by Hiroshima University Hospital. Silk elastin is provided by Sanyo Chemical Industries, Ltd. If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures





References
-
- Askling C.M., Tengvar M., Tarassova O., Thorstensson A. Acute hamstring injuries in Swedish elite sprinters and jumpers: a prospective randomised controlled clinical trial comparing two rehabilitation protocols. Br J Sports Med. 2014;48(7):532–539. - PubMed
-
- Ekstrand J., Hagglund M., Walden M. Epidemiology of muscle injuries in professional football (soccer) Am J Sports Med. 2011;39(6):1226–1232. - PubMed
-
- Gabbe B.J., Bennell K.L., Finch C.F., Wajswelner H., Orchard J.W. Predictors of hamstring injury at the elite level of Australian football. Scand J Med Sci Sports. 2006;16(1):7–13. - PubMed
-
- Ishoi L., Krommes K., Husted R.S., Juhl C.B., Thorborg K. Diagnosis, prevention and treatment of common lower extremity muscle injuries in sport - grading the evidence: a statement paper commissioned by the Danish Society of Sports Physical Therapy (DSSF) Br J Sports Med. 2020;54(9):528–537. - PMC - PubMed
LinkOut - more resources
Full Text Sources
