

Neuroanatomical dimensions in medication-free individuals with major depressive disorder and treatment response to SSRI antidepressant medications or placebo
- PMID: 38948238
- PMCID: PMC11211072
- DOI: 10.1038/s44220-023-00187-w
Neuroanatomical dimensions in medication-free individuals with major depressive disorder and treatment response to SSRI antidepressant medications or placebo
Abstract
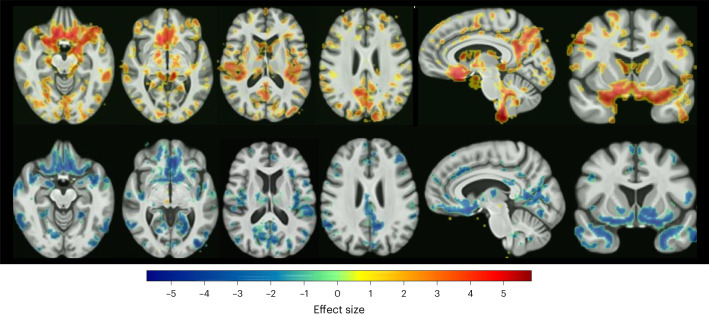
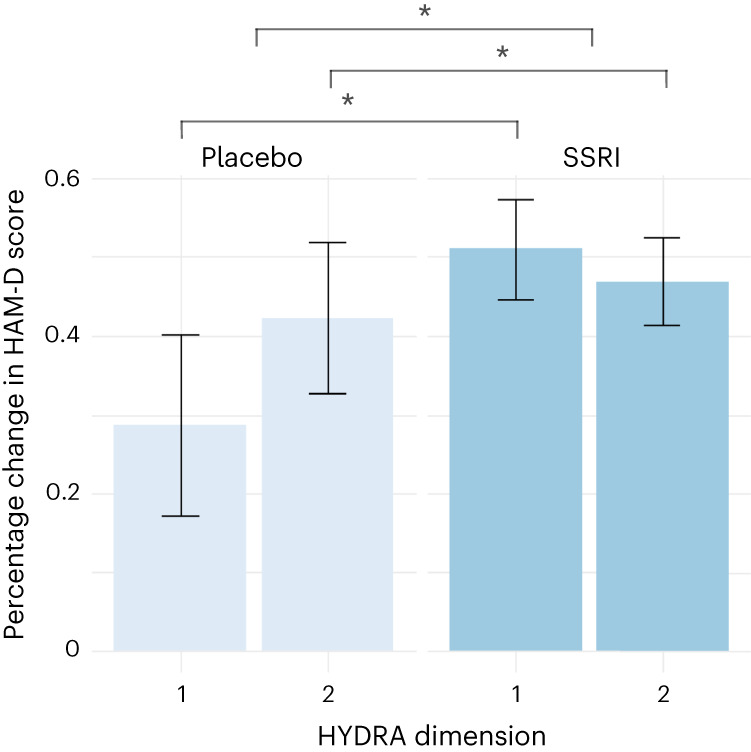
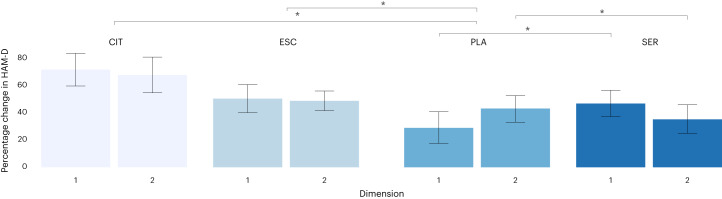
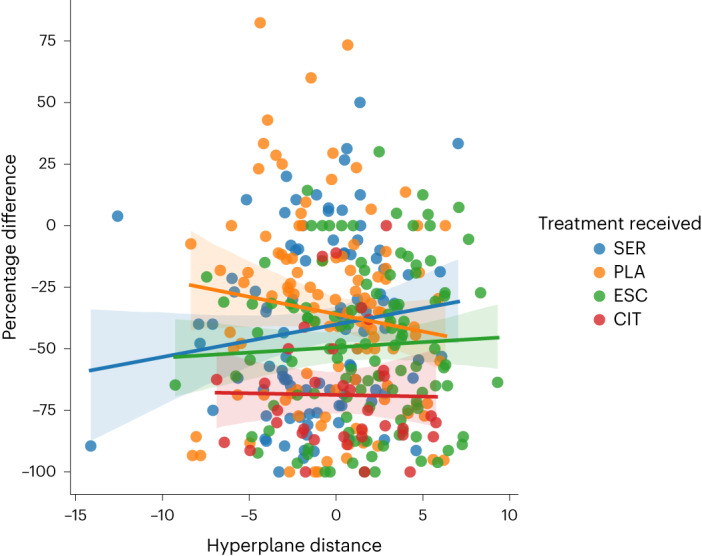
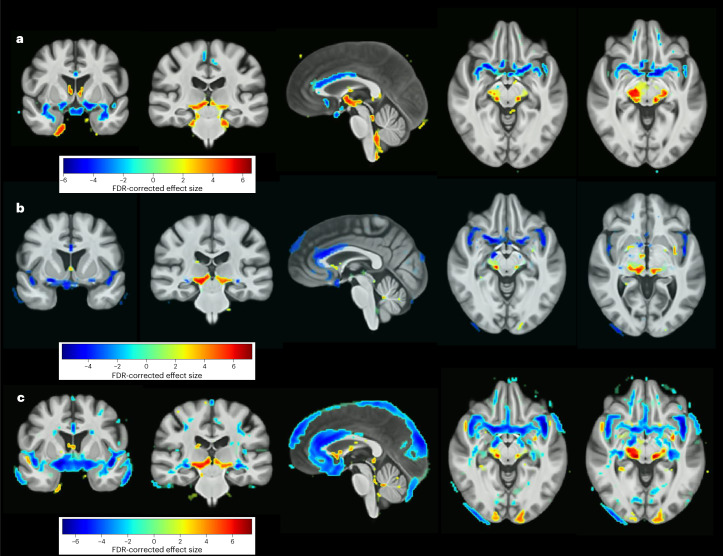
Major depressive disorder (MDD) is a heterogeneous clinical syndrome with widespread subtle neuroanatomical correlates. Our objective was to identify the neuroanatomical dimensions that characterize MDD and predict treatment response to selective serotonin reuptake inhibitor (SSRI) antidepressants or placebo. In the COORDINATE-MDD consortium, raw MRI data were shared from international samples (N = 1,384) of medication-free individuals with first-episode and recurrent MDD (N = 685) in a current depressive episode of at least moderate severity, but not treatment-resistant depression, as well as healthy controls (N = 699). Prospective longitudinal data on treatment response were available for a subset of MDD individuals (N = 359). Treatments were either SSRI antidepressant medication (escitalopram, citalopram, sertraline) or placebo. Multi-center MRI data were harmonized, and HYDRA, a semi-supervised machine-learning clustering algorithm, was utilized to identify patterns in regional brain volumes that are associated with disease. MDD was optimally characterized by two neuroanatomical dimensions that exhibited distinct treatment responses to placebo and SSRI antidepressant medications. Dimension 1 was characterized by preserved gray and white matter (N = 290 MDD), whereas Dimension 2 was characterized by widespread subtle reductions in gray and white matter (N = 395 MDD) relative to healthy controls. Although there were no significant differences in age of onset, years of illness, number of episodes, or duration of current episode between dimensions, there was a significant interaction effect between dimensions and treatment response. Dimension 1 showed a significant improvement in depressive symptoms following treatment with SSRI medication (51.1%) but limited changes following placebo (28.6%). By contrast, Dimension 2 showed comparable improvements to either SSRI (46.9%) or placebo (42.2%) (β = -18.3, 95% CI (-34.3 to -2.3), P = 0.03). Findings from this case-control study indicate that neuroimaging-based markers can help identify the disease-based dimensions that constitute MDD and predict treatment response.
Keywords: Depression; Predictive markers.
© The Author(s) 2024.
Conflict of interest statement
Competing interestsS.R.A. has consulted for Indoc Research Canada. B.W.D. has received research support from Boehringer-Ingelheim, Compass, Pathways, NIMH, Otsuka, and Uson and honoraria for consulting from Aya Biosciences, Myriad Neuroscience, Otsuka, Sophren Therapeutics, Cerebral Therapeutics, Sage. C.H.Y.F. has received grant funding from Brain and Behavior (NARSAD), Eli Lilly and Co. Milken Institute, Flow Neuroscience, MRC, NIMH, Rosetrees Trust, and Wellcome Trust and is Section Editor of Brain Research Bulletin. C.J.H. serves as a consultant for P1vital, Lundbeck, Servier, and Compass Pathways. She holds grant income from Zogenix and J&J. S.H.K. has received funding for consulting or speaking engagements from Abbvie, Boehringer-Ingelheim, Janssen, Lundbeck, Lundbeck Institute, Merck, Otsuka Pfizer, Sunovion, and Servier. He has received research support from Abbott, Brain Canada, CIHR (Canadian Institutes of Health Research), Janssen, Lundbeck, Ontario Brain Institute, Otsuka, Pfizer, and SPOR (Canada’s Strategy for Patient-Oriented Research). He has stock/stock options in Field Trip Health. G.M.K. has received honoraria as a speaker for Sage Biogen and as a consultant for Sanos. H.S.M. has received grant funding from NIH and consulting and IP licenses fees from Abbott Labs. A.M.M. has received research support from Eli Lilly, Janssen, and The Sackler Trust. A.M.M. has also received speaker fees from Illumina and Janssen. W.E.C. serves on the National Advisory Board of the George West Mental health Foundation, as a board member of Hugarheill ehf (an Icelandic company dedicated to the prevention of depression), and on the scientific advisory boards of AIM for Mental Health and the Anxiety and Depression Association of America; he is supported by the Mary and John Brock Foundation, the Pitts Foundation, and the Fuqua family foundations, and he receives book royalties from John Wiley. H.S. has received grant funding from NIH. S.C.S. received research support from Brain Canada, CIHR (Canadian Institutes of Health Research), Ontario Brain Institute, and CFI (Canadian Foundation for Innovation). S.C.S. is a founder and shareholder of ADMdx, Inc. D.T. has received grant funding from NIH. M.H.T. received research support from NIH, PCORI, and AFSP, is a consultant for Alkermes Inc., Alto Neuroscience Inc, Axsome Therapeutics, Boegringer Ingelheim, GH Research, GreenLight VitalSign6 Inc, Heading Health, Inc., Janssen Pharmaceutical, Legion Health, Merck Sharp & Dohme Corp., Mind Medicine Inc., Navitor, Neurocrine Biosciences Inc., Noema Pharma AG, Orexo US Inc., Otsuka Canada Pharmaceutical Inc, Otsuka Pharmaceutical Development & Commercialization, Inc. (MDD section adviser), SAGE Therapeutics, Signant Health, and Takeda Pharmaceuticals Inc and receives editorial compensation from Oxford University Press. A.H.Y. reports the following conflicts of interest: paid lectures and advisory boards for the following companies: Astrazenaca, Eli Lilly, Lundbeck, Sunovion, Servier, Livanova, Janssen, Allegan, Bionomics, Sumitomo Dainippon Pharma, COMPASS, Sage, Novartis; consultant to Johnson & Johnson and to Livanova; received honoraria for attending advisory boards and presenting talks at meetings organized by LivaNova; principal investigator in the Restore-Life VNS registry study funded by LivaNova; UK chief investigator for Novartis MDD study MIJ821A12201; principal investigator on ESKETINTRD3004: ‘An Open-label, Long-term, Safety and Efficacy Study of Intranasal Esketamine in Treatment-resistant Depression’; principal investigator on ‘The Effects of Psilocybin on Cognitive Function in Healthy Participants’; principal investigator on ‘The Safety and Efficacy of Psilocybin in Participants with Treatment-Resistant Depression (P-TRD)’; no shareholdings in pharmaceutical companies; deputy editor of BJPsych Open. Grant funding (past and present): NIMH (USA); CIHR (Canada); NARSAD (USA); Stanley Medical Research Institute (USA); MRC (UK); Wellcome Trust (UK); Royal College of Physicians (Edin); BMA (UK); UBC-VGH Foundation (Canada); WEDC (Canada); CCS Depression Research Fund (Canada); MSFHR (Canada); NIHR (UK); Janssen (UK). R.Z. is a private psychiatrist service provider at The London Depression Institute and co-investigator on a Livanova-funded observational study of vagus nerve stimulation for depression. R.Z. has received honoraria for talks at medical symposia sponsored by Lundbeck as well as Janssen. He has collaborated with EMIS PLC and advises Depsee Ltd. He is affiliated with the D’Or Institute of Research and Education, Rio de Janeiro, and advises the Scients Institute, USA. Authors A. Singh, A. Stolicyn, B.R.G., B.N.F., C.C.F., C.-G.Y., C.D., D.A., D.W., G.E., H.C.W., I.H.G., I.M.A., I.S., J.F.W.D., J.Q., J.S., J.A.G., K.H., K.S.C., K.Q., M.P.P., M.A., M.D.S., M.G., Q.G., R.E., S.H., S.R., T.A.V., T.C., T.W., V.G.F., and Y.F. declare that they have no competing interests.
Figures
References
-
- James, S. L. et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet392, 1789–1858 (2018). 10.1016/S0140-6736(18)32279-7 - DOI - PMC - PubMed
-
- Rush, A. J. The varied clinical presentations of major depressive disorder. J. Clin. Psychiatry.68, 4–10 (2007). - PubMed
Grants and funding
- R01 MH123550/MH/NIMH NIH HHS/United States
- R01 MH112070/MH/NIMH NIH HHS/United States
- R01 MH080880/MH/NIMH NIH HHS/United States
- R01 MH101472/MH/NIMH NIH HHS/United States
- G0902304/MRC_/Medical Research Council/United Kingdom
- RF1 AG054409/AG/NIA NIH HHS/United States
- U01 DA041089/DA/NIDA NIH HHS/United States
- K01 MH096077/MH/NIMH NIH HHS/United States
- MR/T017538/1/MRC_/Medical Research Council/United Kingdom
- R01 MH134236/MH/NIMH NIH HHS/United States
- R01 MH125850/MH/NIMH NIH HHS/United States
- P20 GM121312/GM/NIGMS NIH HHS/United States
- R37 MH101495/MH/NIMH NIH HHS/United States
- R01 EB022573/EB/NIBIB NIH HHS/United States
- R01 MH098099/MH/NIMH NIH HHS/United States
- R01 AG066650/AG/NIA NIH HHS/United States
- U01 AG068057/AG/NIA NIH HHS/United States
- U01 MH092250/MH/NIMH NIH HHS/United States
- P50 MH077083/MH/NIMH NIH HHS/United States
- WT_/Wellcome Trust/United Kingdom
- U01 MH092221/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources