

This is a preprint.
Sex differences and immune correlates of Long COVID development, persistence, and resolution
- PMID: 38948732
- PMCID: PMC11212991
- DOI: 10.1101/2024.06.18.599612
Sex differences and immune correlates of Long COVID development, persistence, and resolution
Update in
-
Sex differences and immune correlates of Long Covid development, symptom persistence, and resolution.Sci Transl Med. 2024 Nov 13;16(773):eadr1032. doi: 10.1126/scitranslmed.adr1032. Epub 2024 Nov 13. Sci Transl Med. 2024. PMID: 39536117 Free PMC article.
Abstract
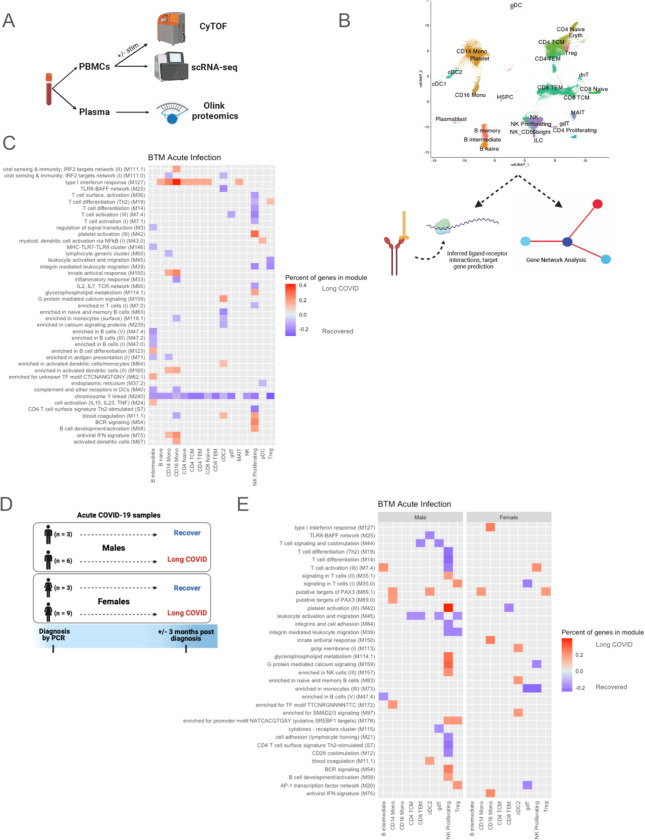
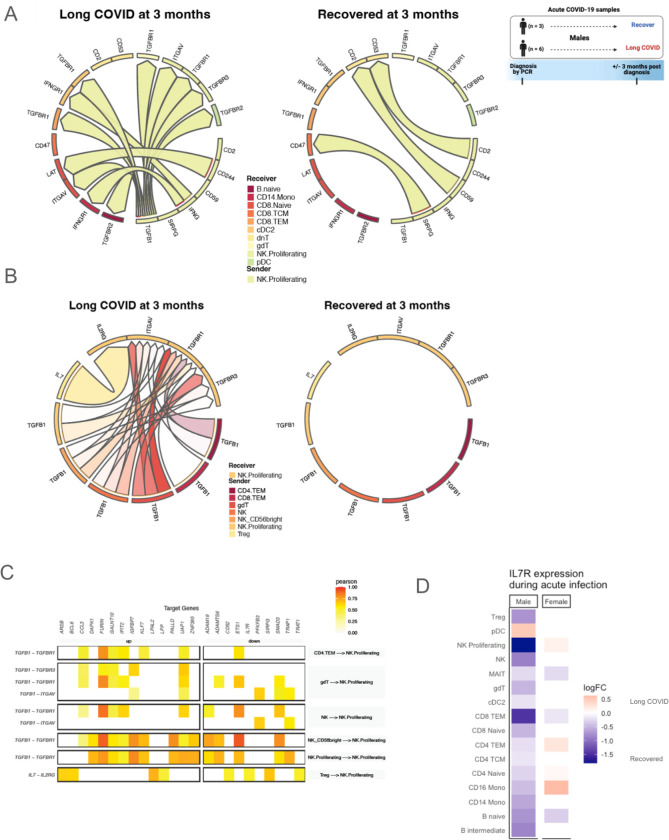
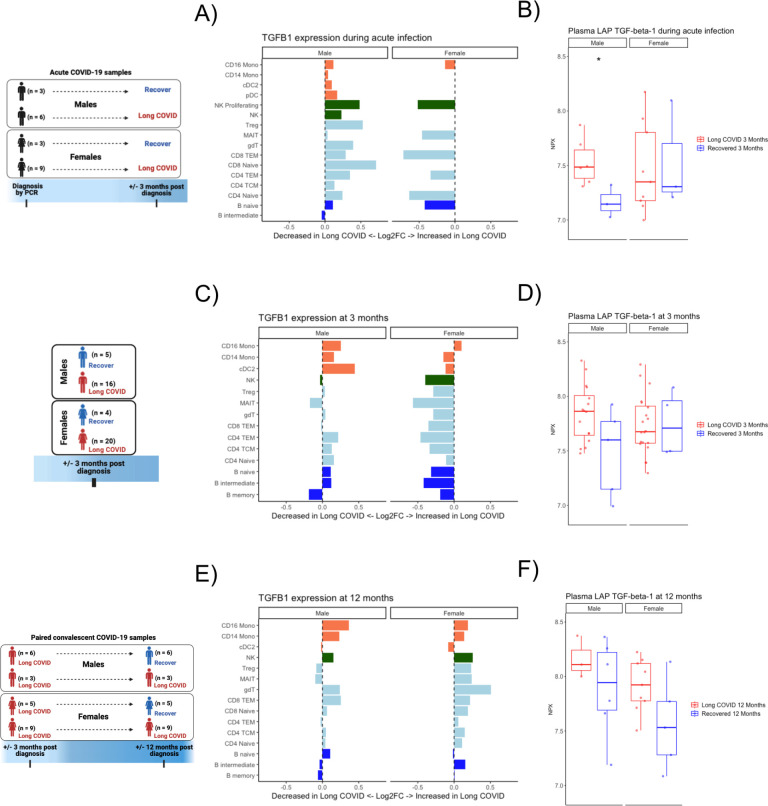
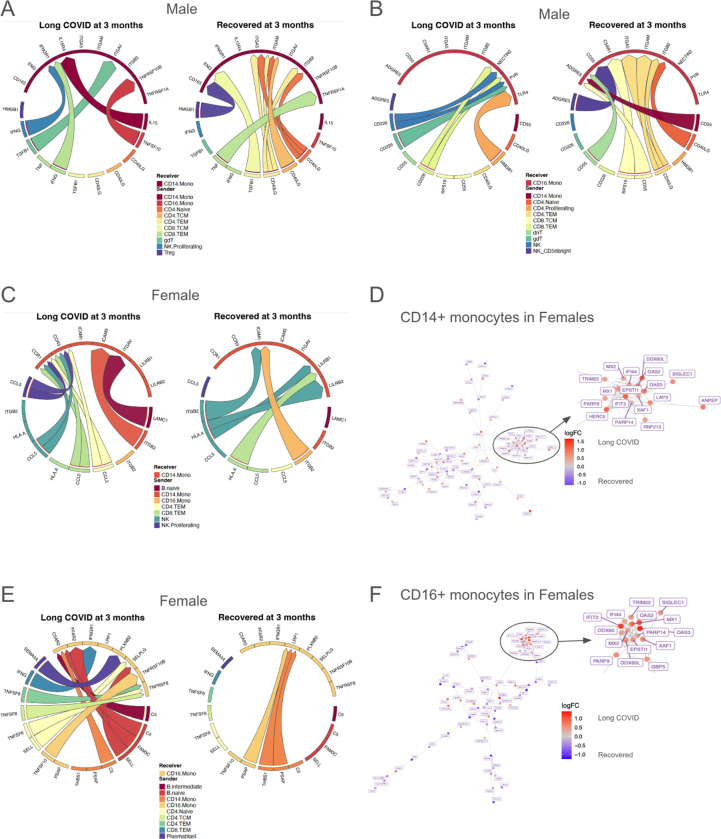
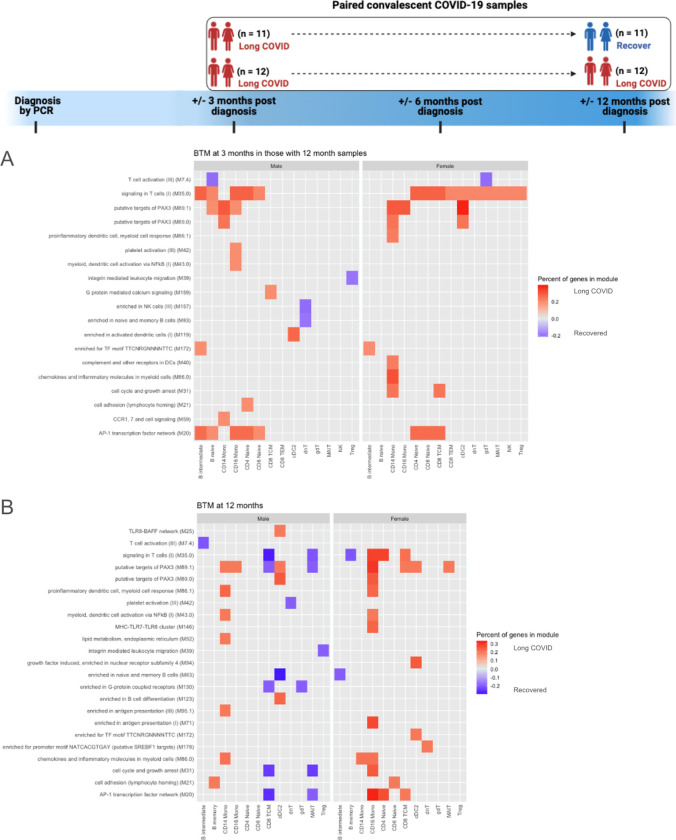
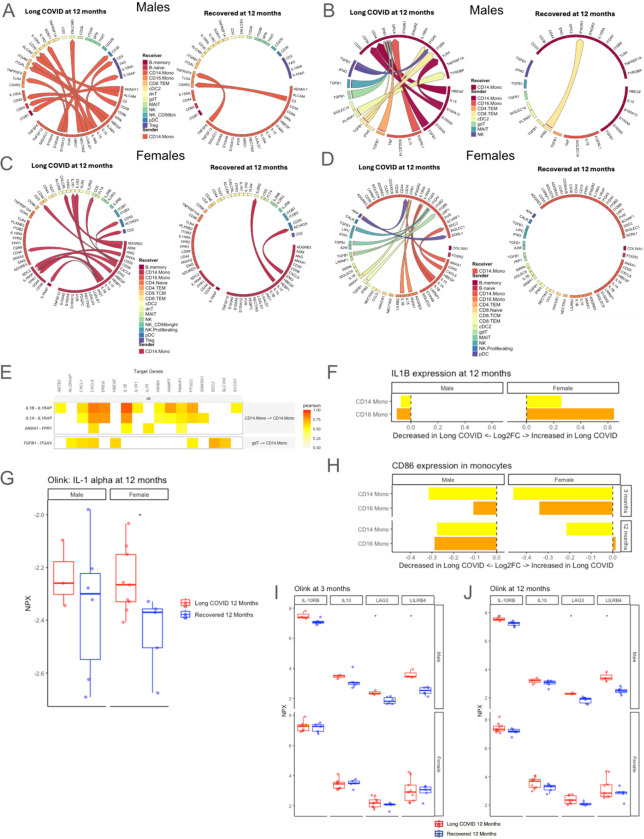
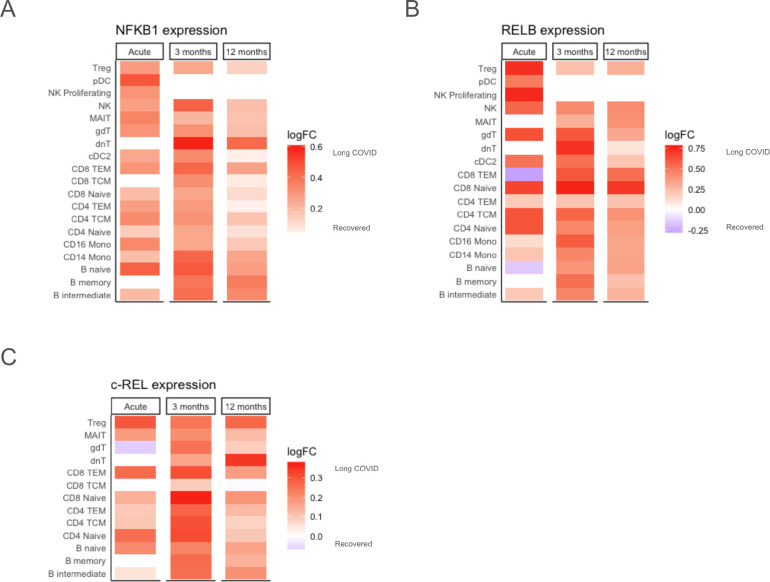
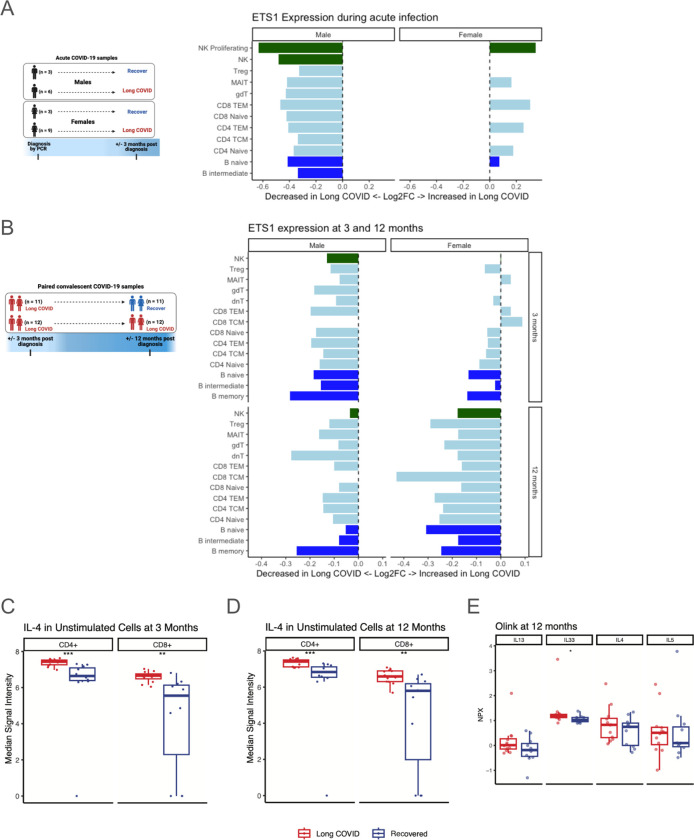
Sex differences have been observed in acute COVID-19 and Long COVID (LC) outcomes, with greater disease severity and mortality during acute infection in males and a greater proportion of females developing LC. We hypothesized that sex-specific immune dysregulation contributes to the pathogenesis of LC. To investigate the immunologic underpinnings of LC development and persistence, we used single-cell transcriptomics, single-cell proteomics, and plasma proteomics on blood samples obtained during acute SARS-CoV-2 infection and at 3 and 12 months post-infection in a cohort of 45 patients who either developed LC or recovered. Several sex-specific immune pathways were associated with LC. Specifically, males who would develop LC at 3 months had widespread increases in TGF-β signaling during acute infection in proliferating NK cells. Females who would develop LC demonstrated increased expression of XIST, an RNA gene implicated in autoimmunity, and increased IL1 signaling in monocytes at 12 months post infection. Several immune features of LC were also conserved across sexes. Both males and females with LC had reduced co-stimulatory signaling from monocytes and broad upregulation of NF-κB transcription factors. In both sexes, those with persistent LC demonstrated increased LAG3, a marker of T cell exhaustion, reduced ETS1 transcription factor expression across lymphocyte subsets, and elevated intracellular IL-4 levels in T cell subsets, suggesting that ETS1 alterations may drive an aberrantly elevated Th2-like response in LC. Altogether, this study describes multiple innate and adaptive immune correlates of LC, some of which differ by sex, and offers insights toward the pursuit of tailored therapeutics.
Conflict of interest statement
Competing interests: Upinder Singh reports research support from National Institutes of Health, Agency for Healthcare Research and Quality, and Pfizer, Inc.; she is an advisor to Regeneron and Gilead. Catherine Blish is an advisor to Immunebridge and DeepCell on topics unrelated to this research. All other authors declare no competing interests.
Figures
References
-
- WHO Coronavirus (COVID-19) Dashboard (available at https://covid19.who.int).
-
- Coronavirus disease (COVID-19): Post COVID-19 condition (available at https://www.who.int/news-room/questions-and-answers/item/coronavirus-dis...).
-
- A. S. for P. Affairs (ASPA), About Long COVID (2023) (available at https://www.covid.gov/be-informed/longcovid/about).
-
- CDC, Healthcare WorkersCent. Dis. Control Prev. (2020) (available at https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-covid-c...).
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous