

Interventional radiology: Diagnosis and treatment of post-traumatic nonischemic priapism: A case report
- PMID: 38948900
- PMCID: PMC11214341
- DOI: 10.1016/j.radcr.2024.05.022
Interventional radiology: Diagnosis and treatment of post-traumatic nonischemic priapism: A case report
Abstract
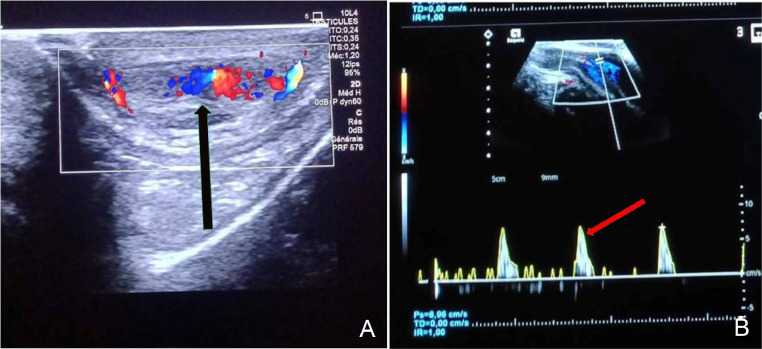
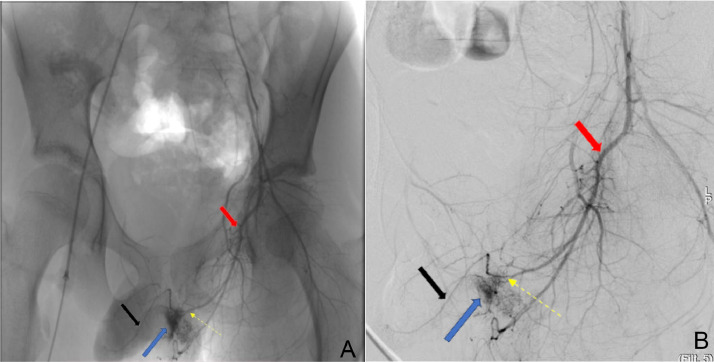
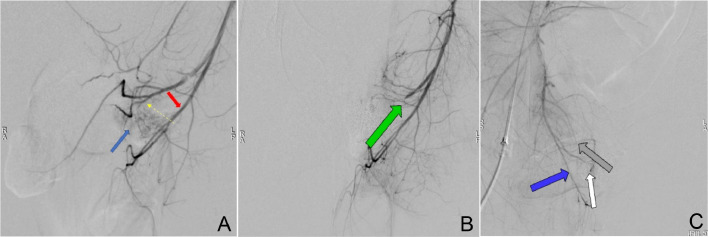
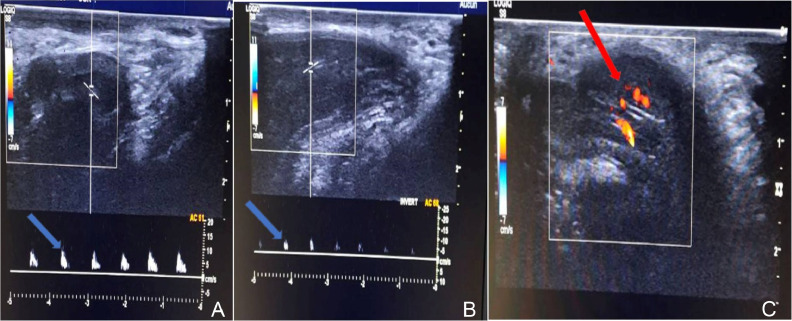
Priapism is defined as a form of erectile dysfunction characterized by a prolonged and involuntary penile erection, either partial or complete, occurring without sexual stimulation and lasting for more than 4 hours. Its incidence is estimated to be 0.5-0.9 cases per 100,000 people per year. The most frequent form is ischemic priapism, results from paralysis of the cavernous smooth muscles, which are unable to contract, leading to the stagnation of hypoxic blood within the sinusoidal spaces. Characterized by a painful rigid and sustainable erection. Non-ischemic priapism constitutes a rare entity, unlike the former, this type is typically painless. It is caused by an excessive influx of blood into the penis without a concomitant increase in outgoing blood flow. Blunt trauma is the most commonly reported etiology. And finally, recurrent priapism is characterized by recurrent episodes of prolonged erection and can be challenging to treat, often requiring long-term management to prevent recurrences. We report a case of high-flow priapism in a 10-year old child, secondary to a cavernous arterial fistula following a straddle injury during sports activity. It was suspected clinically and confirmed by ultrasound-Doppler, then successfully treated radiologically with highly selective embolization, with very satisfactory postoperative outcomes.
Keywords: Arterial embolization; Erectile function; Interventional radiology; Non-ischemic priapism; Penile trauma.
© 2024 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures
Similar articles
-
Successful Management of Recurrent High-Flow Priapism Treated with Selective Arterial Embolization: A Case Report.J Radiol Case Rep. 2023 Nov 30;17(11):18-26. doi: 10.3941/jrcr.v17i11.5230. eCollection 2023 Nov. J Radiol Case Rep. 2023. PMID: 38638553 Free PMC article.
-
Arterial embolization in the treatment of post-traumatic priapism.Ann Urol (Paris). 1999;33(3):210-8. Ann Urol (Paris). 1999. PMID: 10417850
-
Selective Penile Arterial Embolization Preserves Long-Term Erectile Function in Patients with Nonischemic Priapism: An 18-Year Experience.Urology. 2018 Dec;122:116-120. doi: 10.1016/j.urology.2018.07.026. Epub 2018 Jul 29. Urology. 2018. PMID: 30059714
-
Appropriate management of high-flow priapism based on color Doppler ultrasonography findings in pediatric patients: four case reports and a review of the literature.J Pediatr Urol. 2019 Apr;15(2):187.e1-187.e6. doi: 10.1016/j.jpurol.2019.01.005. Epub 2019 Jan 19. J Pediatr Urol. 2019. PMID: 30910454 Review.
-
The role of the urologist in managing high flow priapism.Int J Impot Res. 2025 Feb 5. doi: 10.1038/s41443-025-01017-6. Online ahead of print. Int J Impot Res. 2025. PMID: 39910241 Review.
References
-
- B. Gondran-Tellier, M. André, M. Baboudjian, E. Lechevallier, R. Boissier Le priapisme artériel, progrès en urologie - FMC, 30, 3,2020, F77–F80, ISSN 1761-676X - PubMed
-
- R Carlat, R Destraix, N Jacquemart, F. Melebeck, M. Twahirwa, M De Foy, Un priapisme à haut debit post fracture du bassin revue de: Octobre 2023 Rubrique(s): Chirurgie orthopédique.
-
- Lue TF. In: Campbell's urology. Walsh PC, Retik AB, Vaughan ED, Wein AJ, Kavoussi AR, Novick AC, editors. Saunders; Philadelphia: W.B.: 2002. Physiology of penile erection and pathophysiology of erectile dysfunction and priapism; pp. 1610–1696.
-
- Montague DK, Jarow J, Broderick GA, Dmochowski RR, Heaton JP, Lue TF, Nehra A, Sharlip ID, , Members of the Erectile Dysfunction Guideline Update Panel, & Americal Urological Association American Urological Association guideline on the management of priapism. J Urol. 2003;170(4 Pt 1):1318–1324. doi: 10.1097/01.ju.0000087608.07371.ca. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
