

Traumatic pelvic ring fracture during pregnancy: a systematic review
- PMID: 38949162
- PMCID: PMC11297399
- DOI: 10.1530/EOR-23-0164
Traumatic pelvic ring fracture during pregnancy: a systematic review
Abstract
Purpose: This systematic review aims to investigate the management and outcomes of pelvic ring fractures (PRFs) during pregnancy, emphasizing maternal and fetal mortality rates, mechanisms of injury, and treatment modalities.
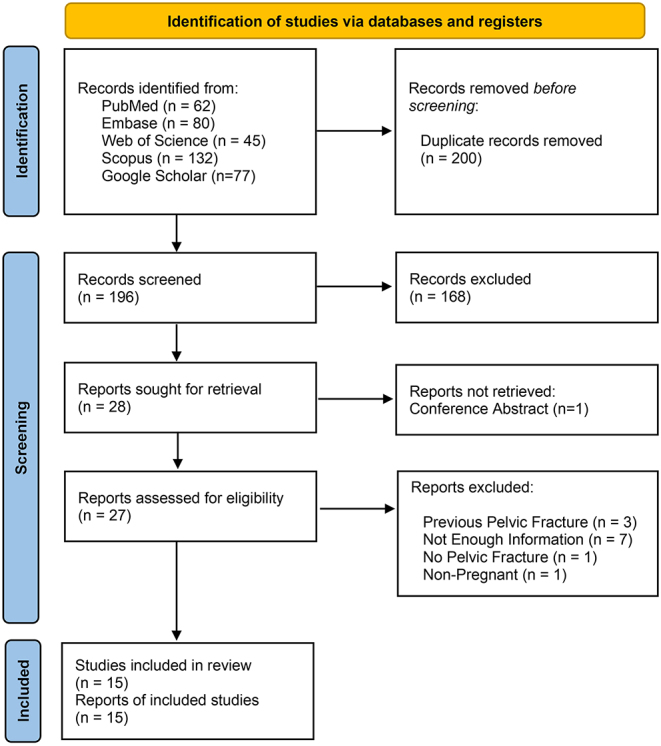
Methods: Following Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, we conducted a comprehensive search of databases from 2000 to 2023, identifying 33 relevant studies. Data extraction included demographics, fracture types, treatment methods, and outcomes. Risk of bias was assessed using the JBI criteria.
Results: Maternal mortality stood at 9.1%, with fetal mortality at 42.4%. Maternal factors impacting mortality included head trauma and hemodynamic instability. Fetal mortality correlated with mechanisms like motor vehicle accidents and maternal vital signs. Surgical and conservative treatments were applied, with a majority of pelvic surgeries performed before delivery. External fixators proved effective in fracture stabilization.
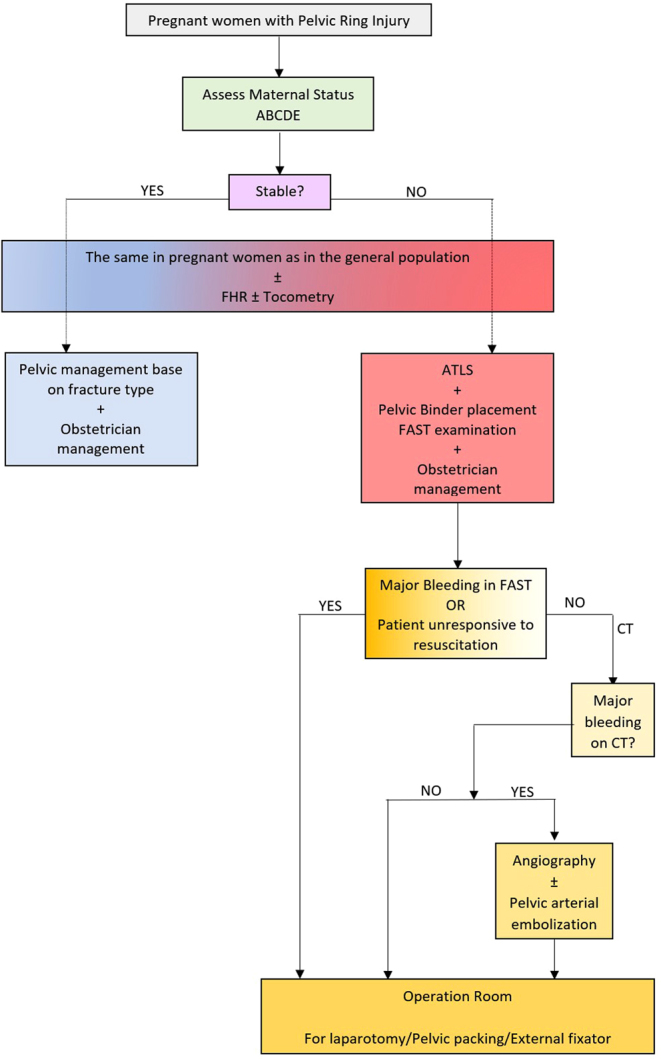
Conclusion: Pelvic ring fractures during pregnancy present significant risks to maternal and fetal health. Early stabilization and vigilant monitoring of maternal vital signs are crucial. Vaginal bleeding/discharge serves as a critical fetal risk indicator. The choice between surgical and conservative treatment minimally influenced outcomes. Multidisciplinary collaboration and tailored interventions are essential in managing these complex cases.
Keywords: external fixators; fetal mortality; fracture types; maternal mortality; pelvic ring fractures; pregnancy; systematic review; treatment.
Conflict of interest statement
Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members.
Figures
Similar articles
-
Pelvic fractures in pregnancy: factors influencing maternal and fetal outcomes.J Trauma. 2002 Oct;53(4):796-804. doi: 10.1097/00005373-200210000-00033. J Trauma. 2002. PMID: 12394889 Review.
-
[Associated injuries in severe pelvic trauma].Unfallchirurg. 2000 Jul;103(7):572-81. doi: 10.1007/s001130050585. Unfallchirurg. 2000. PMID: 10969545 German.
-
Guidelines for the Management of a Pregnant Trauma Patient.J Obstet Gynaecol Can. 2015 Jun;37(6):553-74. doi: 10.1016/s1701-2163(15)30232-2. J Obstet Gynaecol Can. 2015. PMID: 26334607 English, French.
-
Thirty-Day Surgical Morbidity and Mortality in Pelvic and Acetabular Fracture Patients Presenting to a Tertiary Care Hospital in Karachi, Pakistan.Cureus. 2024 Jul 4;16(7):e63801. doi: 10.7759/cureus.63801. eCollection 2024 Jul. Cureus. 2024. PMID: 39099930 Free PMC article.
-
Indications for surgical fixation of low-energy pelvic ring fractures in elderly: a systematic review.Arch Orthop Trauma Surg. 2023 May;143(5):2417-2428. doi: 10.1007/s00402-022-04438-w. Epub 2022 Apr 25. Arch Orthop Trauma Surg. 2023. PMID: 35462589 Free PMC article.
Cited by
-
Fetal radiation during acetabular and pelvic ring fixation: Which injury patterns dictate dangerous levels of fluoroscopic cumulative dose.J Clin Orthop Trauma. 2024 Dec 28;62:102899. doi: 10.1016/j.jcot.2024.102899. eCollection 2025 Mar. J Clin Orthop Trauma. 2024. PMID: 39867590
References
-
- Yoo BJ. Pelvic trauma and the pregnant patient: a review of physiology, treatment risks, and options. Current Trauma Reports 20184225–232. (10.1007/s40719-018-0136-0) - DOI
LinkOut - more resources
Full Text Sources
