

Microsatellite Instability, Tumor Mutational Burden, and Response to Immune Checkpoint Blockade in Patients with Prostate Cancer
- PMID: 38949888
- PMCID: PMC11371520
- DOI: 10.1158/1078-0432.CCR-23-3403
Microsatellite Instability, Tumor Mutational Burden, and Response to Immune Checkpoint Blockade in Patients with Prostate Cancer
Abstract
Purpose: Patients with microsatellite instability-high/mismatch repair-deficient (MSI-H/dMMR) and high tumor mutational burden (TMB-H) prostate cancers are candidates for pembrolizumab. We define the genomic features, clinical course, and response to immune checkpoint blockade (ICB) in patients with MSI-H/dMMR and TMB-H prostate cancers without MSI [TMB-H/microsatellite stable (MSS)].
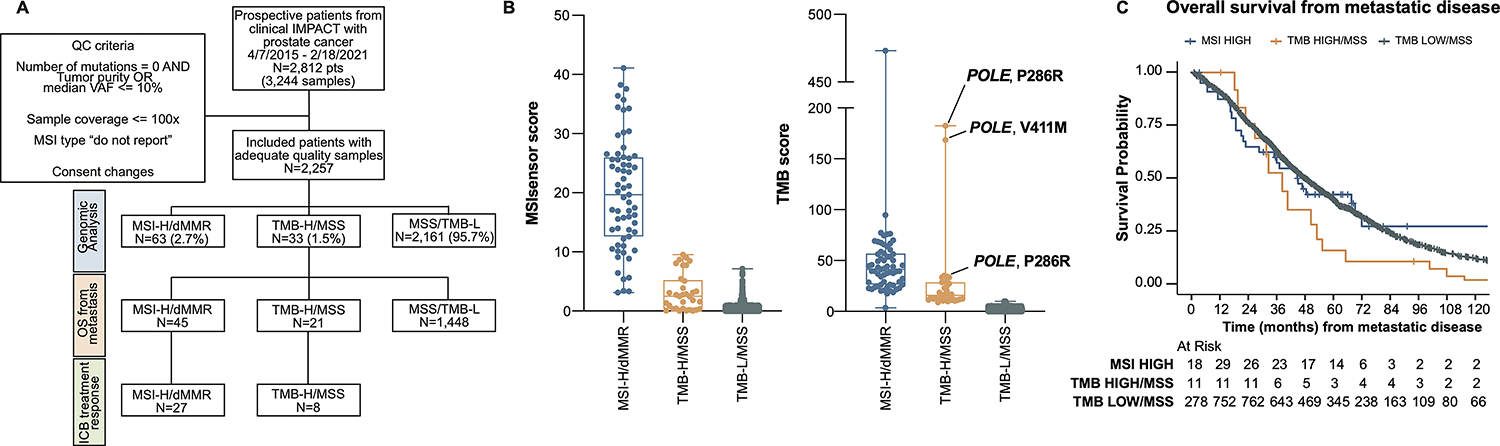
Experimental design: We sequenced 3,244 tumors from 2,257 patients with prostate cancer. MSI-H/dMMR prostate cancer was defined as an MSIsensor score ≥10 or MSIsensor score ≥3 and <10 with a deleterious MMR alteration. TMB-H was defined as ≥10 mutations/megabase. PSA50 and RECIST responses were assigned. Overall survival and radiographic progression-free survival (rPFS) were compared using log-rank test.
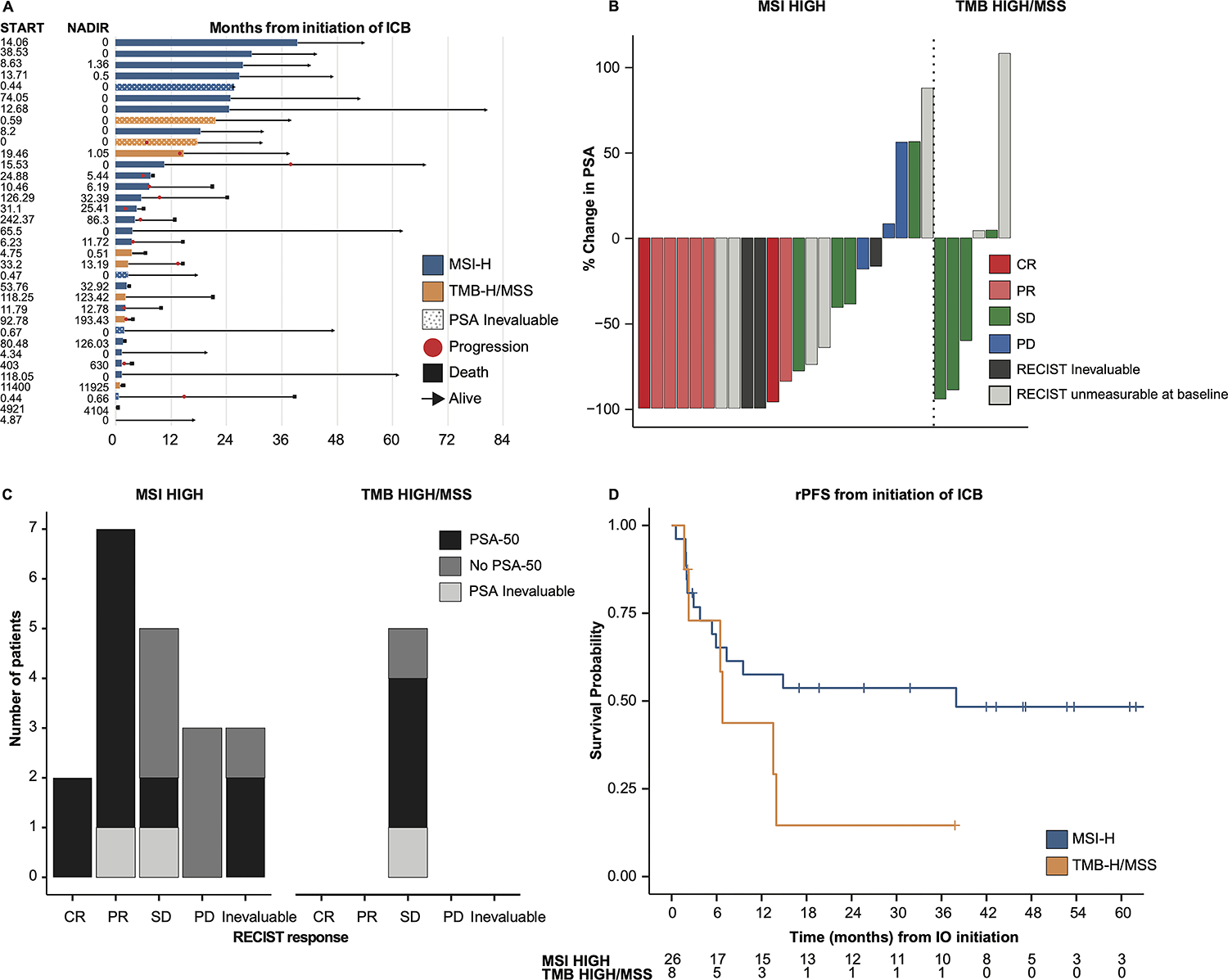
Results: Sixty-three (2.8%) men had MSI-H/dMMR, and 33 (1.5%) had TMB-H/MSS prostate cancers. Patients with MSI-H/dMMR and TMB-H/MSS tumors more commonly presented with grade group 5 and metastatic disease at diagnosis. MSI-H/dMMR tumors had higher TMB, indel, and neoantigen burden compared with TMB-H/MSS. Twenty-seven patients with MSI-H/dMMR and 8 patients with TMB-H/MSS tumors received ICB, none of whom harbored polymerase epsilon (polE) catalytic subunit mutations. About 45% of patients with MSI-H/dMMR had a RECIST response, and 65% had a PSA50 response. No patient with TMB-H/MSS had a RECIST response, and 50% had a PSA50 response. rPFS tended to be longer in patients with MSI-H/dMMR than in patients with TMB-H/MSS who received immunotherapy. Pronounced differences in genomics, TMB, or MSIsensor score were not detected between MSI-H/dMMR responders and nonresponders.
Conclusions: MSI-H/dMMR prostate cancers have greater TMB, indel, and neoantigen burden than TMB-H/MSS prostate cancers, and these differences may contribute to profound and durable responses to ICB.
©2024 American Association for Cancer Research.
Conflict of interest statement
Declaration of Interests:
WA received speaking honoraria from Roche, Pfizer, Medscape, Aptitude Health, Clinical Education Alliance, touchIME and Onclive/MJH Life Sciences, consulting fees from Clovis Oncology, Janssen, ORIC Pharmaceuticals, Daiichi Sankyo and AstraZeneca, and Research Funding (to his institution) from AstraZeneca, Zenith Epigenetics, Clovis Oncology, ORIC Pharmaceuticals, Epizyme, and Nuvation Bio.
D.R. is an uncompensated Advisor and/or Steering Committee member and has received Research Support (PI): Janssen, Astra Zeneca, Bayer, Myovant, Genentech, Promontory, BMS/Celgene
M.F.B. has received consulting fees from Eli Lilly, AstraZeneca, and Paige.AI.
D.B.S. has served as a consultant for/received honorarium from Pfizer, Loxo/Lilly Oncology, Vividion Therapeutics, Scorpion Therapeutics, Fore Therapeutics, FOG Pharma, Rain Therapeutics, Function Oncology, Elsie Biotherapeutics, and BridgeBio.
All other authors have no relevant declarations of interest.
Figures


Comment in
-
Microsatellite instability (MSI) and the tumor mutation burden (TMB) as biomarkers of response to immune checkpoint inhibitors in prostate cancer.Transl Cancer Res. 2025 May 30;14(5):2553-2557. doi: 10.21037/tcr-2024-2516. Epub 2025 May 12. Transl Cancer Res. 2025. PMID: 40530111 Free PMC article. No abstract available.
References
-
- FDA approves pembrolizumab for adults and children with TMB-H solid tumors 2020. https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-pemb....
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
