

Estimated annual healthcare costs after acute pulmonary embolism: results from a prospective multicentre cohort study
- PMID: 38950900
- PMCID: PMC12045087
- DOI: 10.1093/ehjqcco/qcae050
Estimated annual healthcare costs after acute pulmonary embolism: results from a prospective multicentre cohort study
Abstract
Aims: Patients surviving acute pulmonary embolism (PE) necessitate long-term treatment and follow-up. We estimated, the chronic economic impact of PE on the German healthcare system.
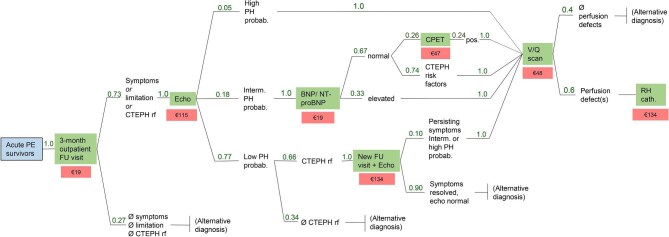
Methods and results: We calculated the direct cost of illness during the first year after discharge for the index PE, analysing data from a multicentre prospective cohort study in Germany. Main and accompanying readmission diagnoses were used to calculate DRG-based hospital reimbursements; anticoagulation costs were estimated from the exact treatment duration and each drug's unique national identifier; and outpatient post-PE care costs from guidelines-recommended algorithms and national reimbursement catalogues. Of 1017 patients enrolled at 17 centres, 958 (94%) completed ≥3-month follow-up; of those, 24% were rehospitalized (0.34 [95% CI 0.30-0.39] readmissions per PE survivor). Age, coronary artery, pulmonary and kidney disease, diabetes, and (in the sensitivity analysis of 837 patients with complete 12-month follow-up) cancer, but not recurrent PE, were independent cost predictors by hurdle gamma regression accounting for zero readmissions. The estimated rehospitalization cost was €1138 (95% CI 896-1420) per patient. Anticoagulation duration was 329 (IQR 142-365) days, with estimated average per-patient costs of €1050 (median 972; IQR 458-1197); costs of scheduled ambulatory follow-up visits amounted to €181. Total estimated direct per-patient costs during the first year after PE ranged from €2369 (primary analysis) to €2542 (sensitivity analysis).
Conclusion: By estimating per-patient costs and identifying cost drivers of post-PE care, our study may inform decisions concerning implementation and reimbursement of follow-up programmes aiming at improved cardiovascular prevention.
Keywords: Anticoagulation; Cost of illness; Economic burden; Long-term care; Pulmonary embolism; Readmission.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
K.M., P.M., T.N., K.C.C., I.T.F., K.K. (Kaier), K.K. (Keller), D.B., C.A., L.B., I.S., H.B., and L.V.: no disclosures; S.B.: Boston Scientific, Medtronic, Bayer, sanofi, institutional research support by Board; Boston Scientific, Penumbra, Viatris, personal fees/honoraria; R.E.: Janssen, OMT, Astra-Zeneca, Novartis, Boehringer-Ingelheim, AOP, LungPacer personal lecture/consultant fees; F.K.: research support from Bayer, BMS, BSCI, AstraZeneca, MSD, Leo Pharma, Actelion, Farm-X, The Netherlands Organization for Health Research and Development, The Dutch Thrombosis Foundation, The Dutch Heart Foundation and the Horizon Europe Program, all outside this manuscript and paid to his institution.; L.H.: MSD, Janssen, Inari Medical, personal lecture/consultant fees; P.S.W.: research funding from Bayer AG for the FOCUS BioSeq Study and outside the submitted work, consulting fees from Astra Zeneca, research funding from Bayer AG, research funding, consulting and lecturing fees from Bayer Health Care, lecturing fees from Bristol Myers Squibb, research funding and consulting fees from Boehringer Ingelheim, research funding and consulting fees from Daiichi Sankyo Europe, consulting fees and non-financial support from Diasorin, non-financial research support from I.E.M., research funding and consulting fees from Novartis Pharma, lecturing fees from Pfizer Pharma, non-financial grants from Philips Medical Systems, research funding and consulting fees from sanofi-aventis. He is principal investigator of the future cluster ‘curATime’ (BMBF 03ZU1202AA, 03ZU1202CD, 03ZU1202DB, 03ZU1202JC, 03ZU1202KB, 03ZU1202LB, 03ZU1202MB, and 03ZU1202OA) and principal investigator of the DIASyM research core (BMBF 161L0217A), and principal investigator of the DZHK (German Center for Cardiovascular Research), Partner Site Rhine-Main, Mainz, Germany; S.R.: remuneration for lectures and/or consultancy from Abbott, Acceleron, Actelion, Aerovate, Altavant, AOP, AstraZeneca, Bayer, Bristol-Myers Squibb, Boehringer-Ingelheim, Edwards, Ferrer, Gossamer, Inari, Janssen, Lilly, MSD, Novartis, Pfizer, and United Therapeutics; and research support to his institution from Actelion, AstraZeneca, Bayer, and Janssen; S.K.: Bayer AG, Boston Scientific, Daiichi-Sankyo, LumiraDx, Penumbra, Inari Medical, personal lecture/advisory fees and research grants to institution; MSD, Pfizer—Bristol-Myers Squibb, personal lecture/advisory fees.
Figures


References
-
- Barco S, Mahmoudpour SH, Valerio L, Klok FA, Münzel T, Middeldorp S et al. Trends in mortality related to pulmonary embolism in the European Region, 2000-15: analysis of vital registration data from the WHO Mortality Database. Lancet Respir Med 2020;8:277–287. 10.1016/S2213-2600(19)30354-6 - DOI - PubMed
-
- Barco S, Valerio L, Ageno W, Cohen AT, Goldhaber SZ, Hunt BJ et al. Age-sex specific pulmonary embolism-related mortality in the USA and Canada, 2000-18: an analysis of the WHO Mortality Database and of the CDC Multiple Cause of Death database. Lancet Respir Med 2021;9:33–42. 10.1016/S2213-2600(20)30417-3 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
