

Low-intensity pulsed ultrasound improves myocardial ischaemia‒reperfusion injury via migrasome-mediated mitocytosis
- PMID: 38951127
- PMCID: PMC11216834
- DOI: 10.1002/ctm2.1749
Low-intensity pulsed ultrasound improves myocardial ischaemia‒reperfusion injury via migrasome-mediated mitocytosis
Abstract
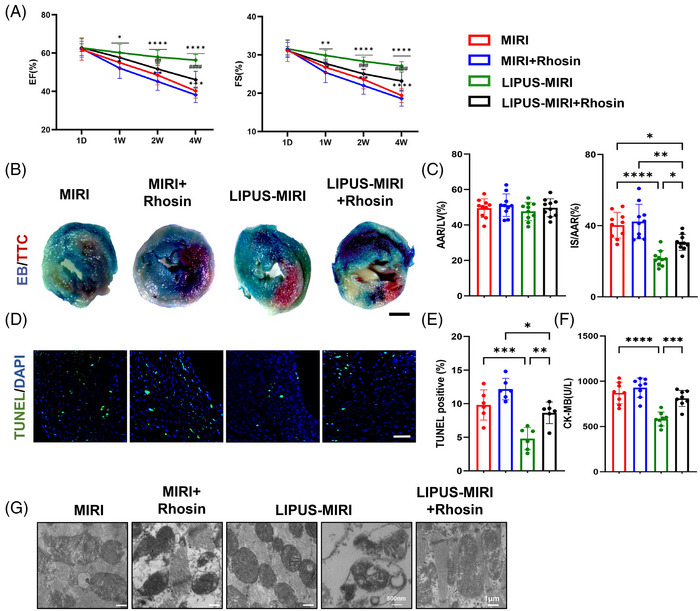
During myocardial ischaemia‒reperfusion injury (MIRI), the accumulation of damaged mitochondria could pose serious threats to the heart. The migrasomes, newly discovered mitocytosis-mediating organelles, selectively remove damaged mitochondria to provide mitochondrial quality control. Here, we utilised low-intensity pulsed ultrasound (LIPUS) on MIRI mice model and demonstrated that LIPUS reduced the infarcted area and improved cardiac dysfunction. Additionally, we found that LIPUS alleviated MIRI-induced mitochondrial dysfunction. We provided new evidence that LIPUS mechanical stimulation facilitated damaged mitochondrial excretion via migrasome-dependent mitocytosis. Inhibition the formation of migrasomes abolished the protective effect of LIPUS on MIRI. Mechanistically, LIPUS induced the formation of migrasomes by evoking the RhoA/Myosin II/F-actin pathway. Meanwhile, F-actin activated YAP nuclear translocation to transcriptionally activate the mitochondrial motor protein KIF5B and Drp1, which are indispensable for LIPUS-induced mitocytosis. These results revealed that LIPUS activates mitocytosis, a migrasome-dependent mitochondrial quality control mechanism, to protect against MIRI, underlining LIPUS as a safe and potentially non-invasive treatment for MIRI.
Keywords: low‐intensity pulsed ultrasound; mitochondria; mitocytosis; myocardial ischaemia‒reperfusion injury.
© 2024 The Author(s). Clinical and Translational Medicine published by John Wiley & Sons Australia, Ltd on behalf of Shanghai Institute of Clinical Bioinformatics.
Conflict of interest statement
The authors declare they have no conflicts of interest.
Figures






References
-
- Reed GW, Rossi JE, Cannon CP. Acute myocardial infarction. Lancet. 2017;389(10065):197‐210. - PubMed
-
- Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics—2022 update: a report from the American Heart Association. Circulation. 2022;145(8):e153‐e639. - PubMed
-
- Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST‐segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST‐segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119‐177. - PubMed
-
- Heusch G. Myocardial ischaemia‒reperfusion injury and cardioprotection in perspective. Nat Rev Cardiol. 2020;17(12):773‐789. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous