

Successful Second Awake Craniotomy Reoperation With Dexmedetomidine After an Initial Abandonment Case Due to Restlessness
- PMID: 38952610
- PMCID: PMC11216107
- DOI: 10.7759/cureus.61506
Successful Second Awake Craniotomy Reoperation With Dexmedetomidine After an Initial Abandonment Case Due to Restlessness
Abstract
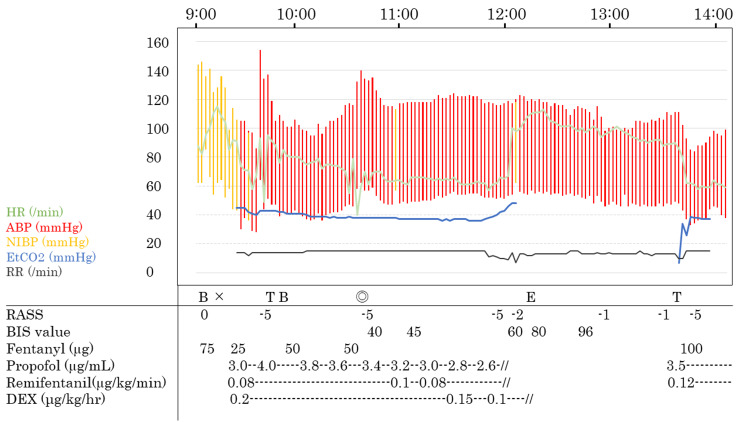
Awake craniotomy (AC) is sometimes aborted due to poor arousal and restlessness. Dexmedetomidine (DEX), an α2-adrenoreceptor agonist, has sedative, analgesic, and anesthetic-sparing effects, with a low risk of respiratory depression, making it effective for intraoperative pain and agitation during the awake phase. We report a case in which AC was successfully performed in combination with low-dose continuous administration of DEX during reoperation in a patient who experienced poor arousal and restlessness during their first surgery, leading to the abandonment of AC. The patient is a 48-year-old male who is scheduled for AC reoperation. Two years ago, the first AC was scheduled and performed under anesthesia with propofol and remifentanil. However, AC was abandoned due to poor intraoperative arousal and restlessness. At reoperation, general anesthesia was induced with propofol and continuous administration of remifentanil (0.1 µg/kg/min); following anesthesia induction (continuous infusion of propofol, remifentanil, and a bolus infusion of fentanyl), DEX was also administered (0.2 µg/kg/hour). We performed a scalp nerve block. Before the awake phase, the propofol dose was decreased as was DEX to 0.1 µg/kg/hour, and propofol and remifentanil were discontinued. The patient gradually awoke without any agitation and restlessness 24 min after stopping propofol and remifentanil and could perform language tasks without any complications. In this case, AC was successfully performed in combination with continuous low-dose administration of DEX at the time of reoperation in a patient who experienced poor arousal and restlessness during their first operation and had to discontinue AC.
Keywords: asleep-awake-awake methods; awake craniotomy; dexmedetomidine; propofol; restlessness.
Copyright © 2024, Ikki et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Institutional Review Board at Nagoya University Hospital issued approval 2023-0459. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Dexmedetomidine as adjunct in awake craniotomy - improvement or not?Anaesthesiol Intensive Ther. 2020;52(1):15-22. doi: 10.5114/ait.2020.93043. Anaesthesiol Intensive Ther. 2020. PMID: 32090308 Free PMC article.
-
Comparison of dexmedetomidine and propofol for conscious sedation in awake craniotomy: a prospective, double-blind, randomized, and controlled clinical trial.Ann Pharmacother. 2013 Nov;47(11):1391-9. doi: 10.1177/1060028013504082. Epub 2013 Nov 5. Ann Pharmacother. 2013. PMID: 24259599 Clinical Trial.
-
Successful Anesthetic Management Using Dexmedetomidine Sequentially with Propofol in the Asleep-Awake-Asleep Technique for Elderly Patients Undergoing Awake Craniotomy.Case Rep Anesthesiol. 2020 Mar 27;2020:6795363. doi: 10.1155/2020/6795363. eCollection 2020. Case Rep Anesthesiol. 2020. PMID: 32280546 Free PMC article.
-
Awake craniotomies in the pediatric population: a systematic review.J Neurosurg Pediatr. 2023 Jun 30;32(4):428-436. doi: 10.3171/2023.4.PEDS22296. Print 2023 Oct 1. J Neurosurg Pediatr. 2023. PMID: 37410631
-
Comparison of dexmedetomidine and propofol for sedation in awake craniotomy: A meta-analysis.Clin Neurol Neurosurg. 2023 Mar;226:107623. doi: 10.1016/j.clineuro.2023.107623. Epub 2023 Feb 9. Clin Neurol Neurosurg. 2023. PMID: 36791589 Review.
References
-
- Failed awake craniotomy: a retrospective analysis in 424 patients undergoing craniotomy for brain tumor. Nossek E, Matot I, Shahar T, et al. J Neurosurg. 2013;118:243–249. - PubMed
-
- Pharmacology of sedative-analgesic agents: dexmedetomidine, remifentanil, ketamine, volatile anesthetics, and the role of peripheral Mu antagonists. Panzer O, Moitra V, Sladen RN. https://doi.org/10.1016/j.anclin.2011.09.002. Anesthesiol Clin. 2011;29:587-605, vii. - PubMed
-
- Clinical pharmacokinetics and pharmacodynamics of dexmedetomidine. Weerink MA, Struys MM, Hannivoort LN, Barends CR, Absalom AR, Colin P. https://doi.org/10.1007/s40262-017-0507-7. Clin Pharmacokinet. 2017;56:893–913. - PMC - PubMed
-
- Conscious sedation with dexmedetomidine compared with asleep-awake-asleep craniotomies in glioma surgery: an analysis of 180 patients. Suero Molina E, Schipmann S, Mueller I, et al. https://doi.org/10.3171/2017.7.JNS171312. J Neurosurg. 2018;129:1223–1230. - PubMed
-
- Management of anesthesia in awake craniotomy. Piccioni F, Fanzio M. https://pubmed.ncbi.nlm.nih.gov/18612268/ Minerva Anestesiol. 2008;74:393–408. - PubMed
Publication types
LinkOut - more resources
Full Text Sources