

Effects of exoskeleton-assisted walking on bowel function in motor-complete spinal cord injury patients: involvement of the brain-gut axis, a pilot study
- PMID: 38952922
- PMCID: PMC11215087
- DOI: 10.3389/fnins.2024.1395671
Effects of exoskeleton-assisted walking on bowel function in motor-complete spinal cord injury patients: involvement of the brain-gut axis, a pilot study
Abstract
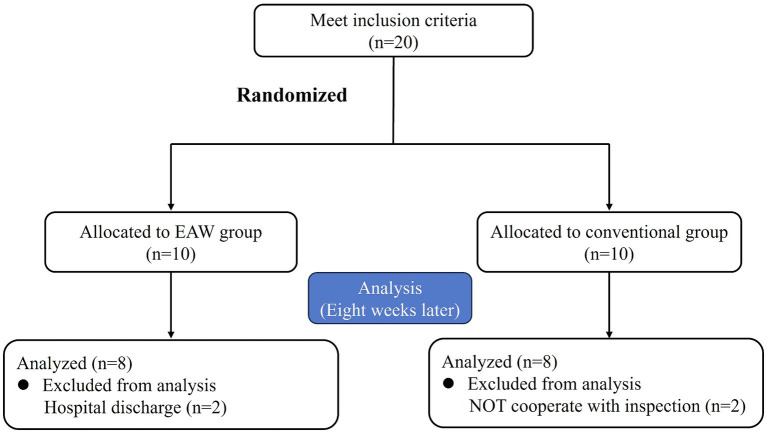
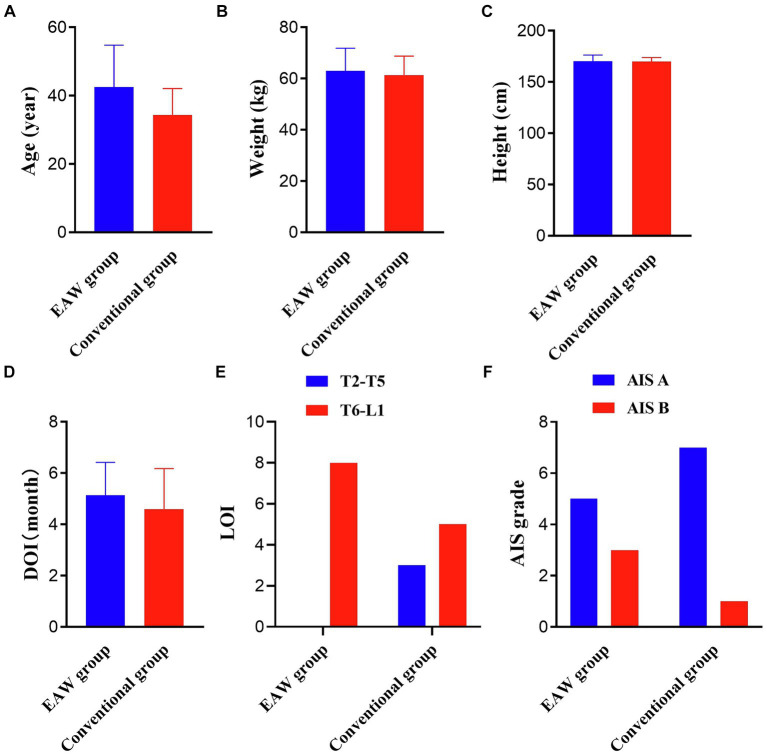
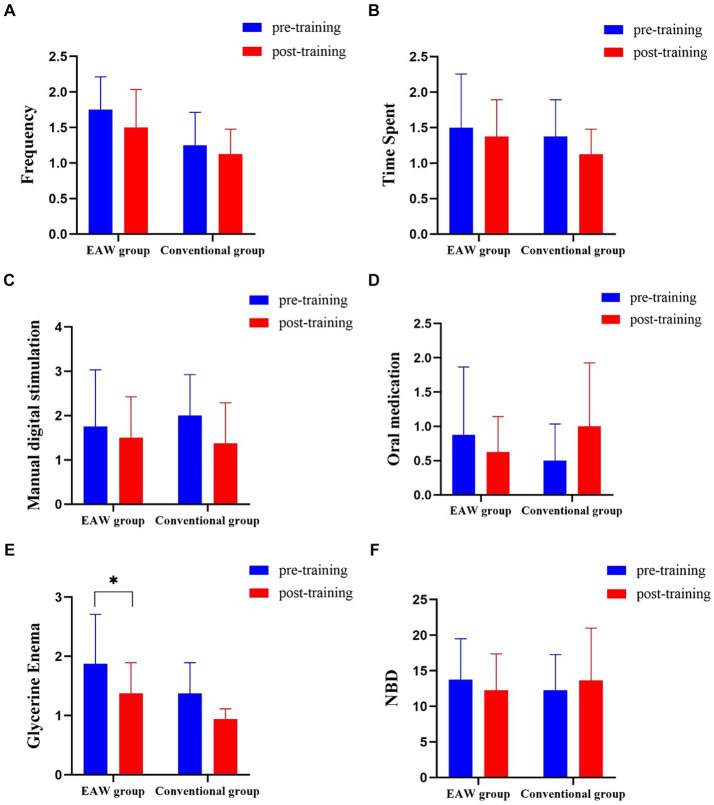
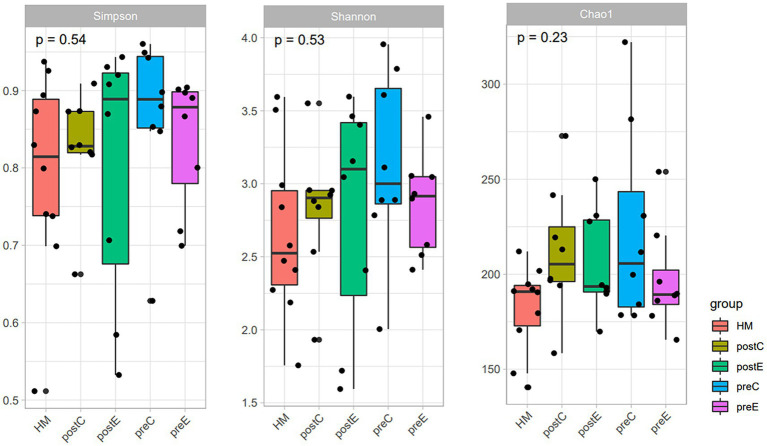
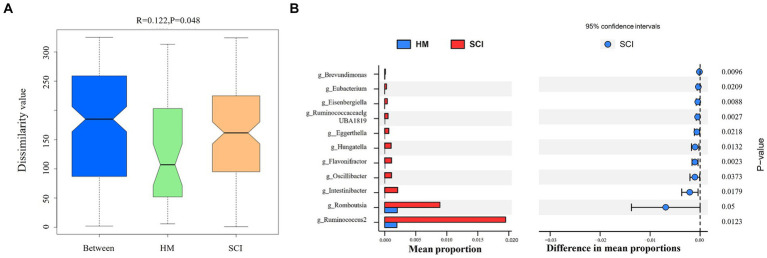
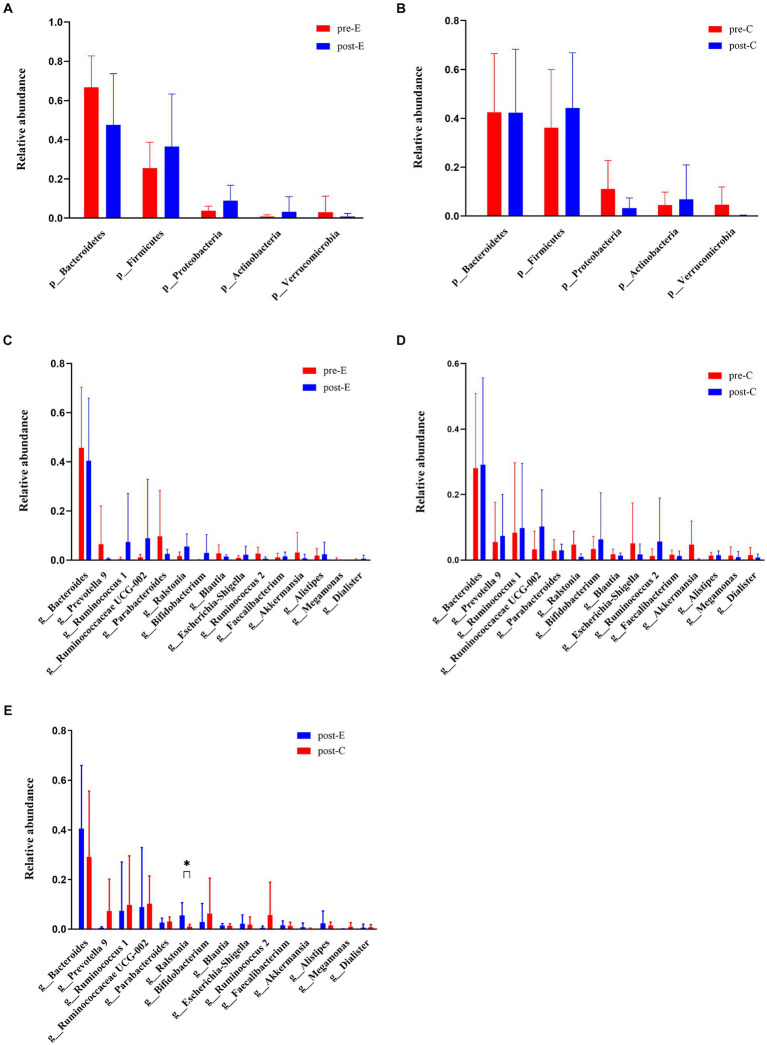
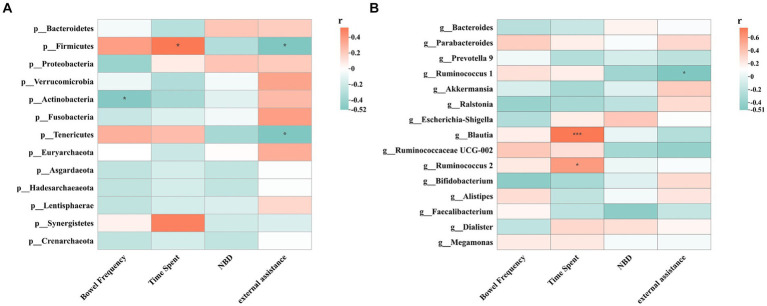
Evidence has demonstrated that exoskeleton robots can improve intestinal function in patients with spinal cord injury (SCI). However, the underlying mechanisms remain unelucidated. This study investigated the effects of exoskeleton-assisted walking (EAW) on intestinal function and intestinal flora structure in T2-L1 motor complete paraplegia patients. The results showed that five participants in the EAW group and three in the conventional group reported improvements in at least one bowel management index, including an increased frequency of bowel evacuations, less time spent on bowel management per day, and less external assistance (manual digital stimulation, medication, and enema usage). After 8 weeks of training, the amount of glycerol used in the EAW group decreased significantly (p <0.05). The EAW group showed an increasing trend in the neurogenic bowel dysfunction (NBD) score after 8 weeks of training, while the conventional group showed a worsening trend. Patients who received the EAW intervention exhibited a decreased abundance of Bacteroidetes and Verrucomicrobia, while Firmicutes, Proteobacteria, and Actinobacteria were upregulated. In addition, there were decreases in the abundances of Bacteroides, Prevotella, Parabacteroides, Akkermansia, Blautia, Ruminococcus 2, and Megamonas. In contrast, Ruminococcus 1, Ruminococcaceae UCG002, Faecalibacterium, Dialister, Ralstonia, Escherichia-Shigella, and Bifidobacterium showed upregulation among the top 15 genera. The abundance of Ralstonia was significantly higher in the EAW group than in the conventional group, and Dialister increased significantly in EAW individuals at 8 weeks. This study suggests that EAW can improve intestinal function of SCI patients in a limited way, and may be associated with changes in the abundance of intestinal flora, especially an increase in beneficial bacteria. In the future, we need to further understand the changes in microbial groups caused by EAW training and all related impact mechanisms, especially intestinal flora metabolites. Clinical trial registration: https://www.chictr.org.cn/.
Keywords: bowel function; constipation; exoskeleton; gut microbiota; spinal cord injury.
Copyright © 2024 Hu, Feng, Lu, Pang, Zhang, Liu, Gou, Bai, Wang, Chang, Yin, Wang, Xiao, Wang, Cheng, Chang and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Changes in bowel function following exoskeletal-assisted walking in persons with spinal cord injury: an observational pilot study.Spinal Cord. 2020 Apr;58(4):459-466. doi: 10.1038/s41393-019-0392-z. Epub 2019 Dec 10. Spinal Cord. 2020. PMID: 31822808 Free PMC article.
-
Exoskeleton-assisted walking improves pulmonary function and walking parameters among individuals with spinal cord injury: a randomized controlled pilot study.J Neuroeng Rehabil. 2021 May 24;18(1):86. doi: 10.1186/s12984-021-00880-w. J Neuroeng Rehabil. 2021. PMID: 34030720 Free PMC article. Clinical Trial.
-
Exoskeleton Training and Trans-Spinal Stimulation for Physical Activity Enhancement After Spinal Cord Injury (EXTra-SCI): An Exploratory Study.Front Rehabil Sci. 2022 Jan;2:789422. doi: 10.3389/fresc.2021.789422. Epub 2022 Jan 4. Front Rehabil Sci. 2022. PMID: 35169770 Free PMC article.
-
Comparison of Efficacy of Lokomat and Wearable Exoskeleton-Assisted Gait Training in People With Spinal Cord Injury: A Systematic Review and Network Meta-Analysis.Front Neurol. 2022 Apr 13;13:772660. doi: 10.3389/fneur.2022.772660. eCollection 2022. Front Neurol. 2022. PMID: 35493806 Free PMC article.
-
Changes of potential shorty-chain fatty acids producing bacteria in the gut of patients with spinal cord injury: a systematic review and meta-analysis.Front Microbiol. 2025 Feb 27;16:1483794. doi: 10.3389/fmicb.2025.1483794. eCollection 2025. Front Microbiol. 2025. PMID: 40083777 Free PMC article.
Cited by
-
An Updated and Comprehensive Review Exploring the Gut-Brain Axis in Neurodegenerative Disorders and Neurotraumas: Implications for Therapeutic Strategies.Brain Sci. 2025 Jun 18;15(6):654. doi: 10.3390/brainsci15060654. Brain Sci. 2025. PMID: 40563824 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources