

Multisite Validation of a Functional Assay to Adjudicate SCN5A Brugada Syndrome-Associated Variants
- PMID: 38953211
- PMCID: PMC11335442
- DOI: 10.1161/CIRCGEN.124.004569
Multisite Validation of a Functional Assay to Adjudicate SCN5A Brugada Syndrome-Associated Variants
Abstract
Background: Brugada syndrome is an inheritable arrhythmia condition that is associated with rare, loss-of-function variants in SCN5A. Interpreting the pathogenicity of SCN5A missense variants is challenging, and ≈79% of SCN5A missense variants in ClinVar are currently classified as variants of uncertain significance. Automated patch clamp technology enables high-throughput functional studies of ion channel variants and can provide evidence for variant reclassification.
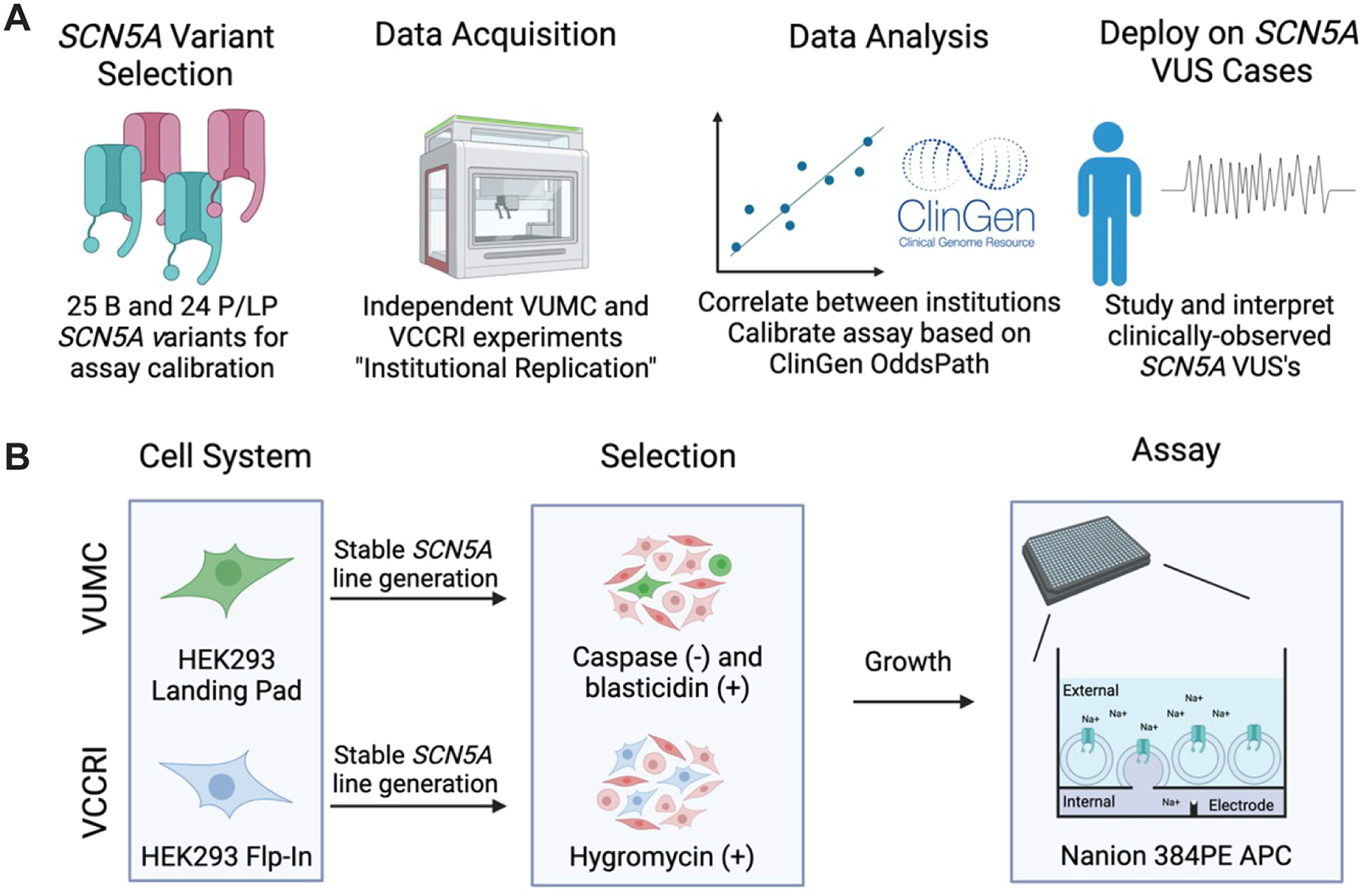
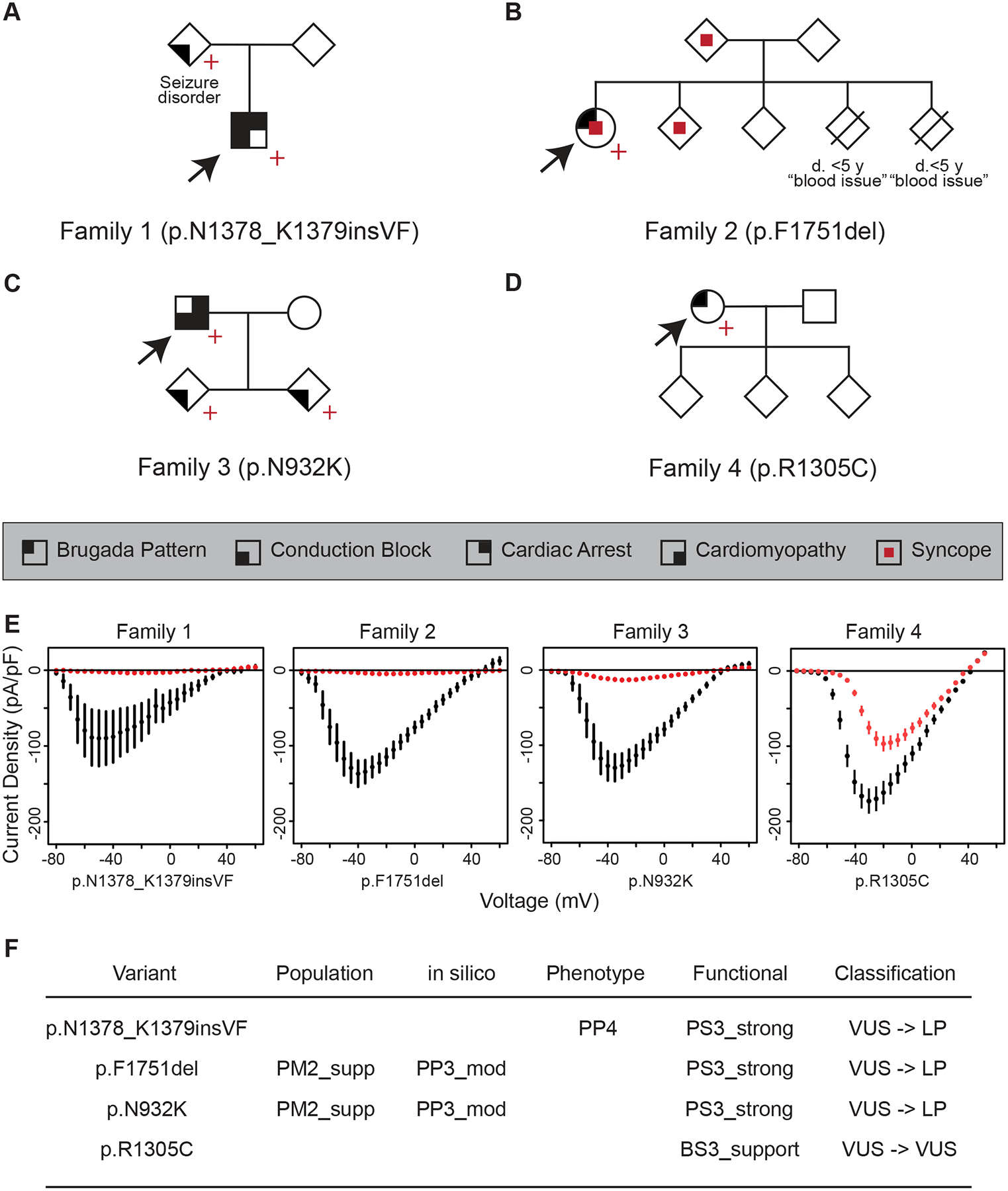
Methods: An in vitro SCN5A-Brugada syndrome automated patch clamp assay was independently performed at Vanderbilt University Medical Center and Victor Chang Cardiac Research Institute. The assay was calibrated according to ClinGen Sequence Variant Interpretation recommendations using high-confidence variant controls (n=49). Normal and abnormal ranges of function were established based on the distribution of benign variant assay results. Odds of pathogenicity values were derived from the experimental results according to ClinGen Sequence Variant Interpretation recommendations. The calibrated assay was then used to study SCN5A variants of uncertain significance observed in 4 families with Brugada syndrome and other arrhythmia phenotypes associated with SCN5A loss-of-function.
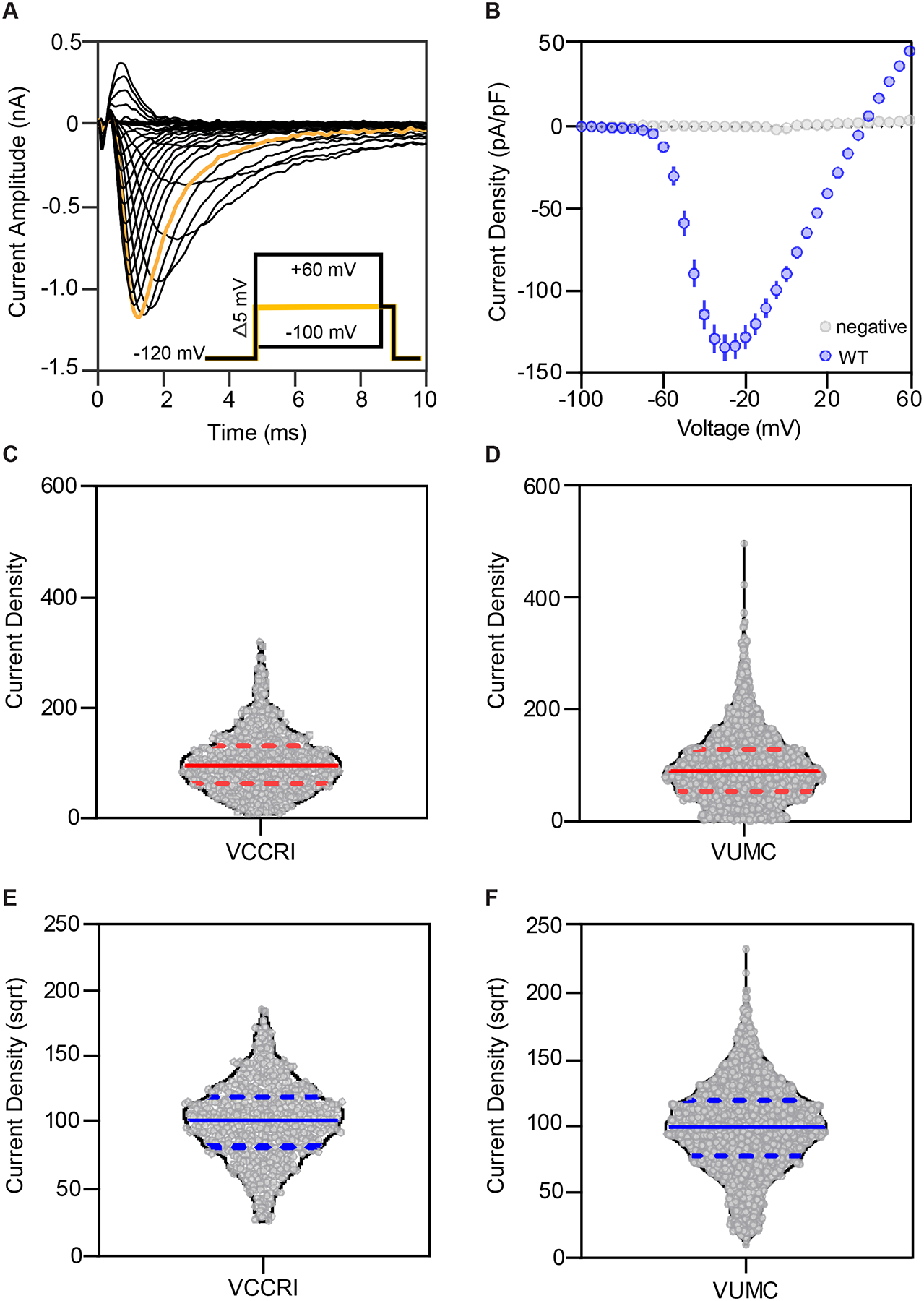
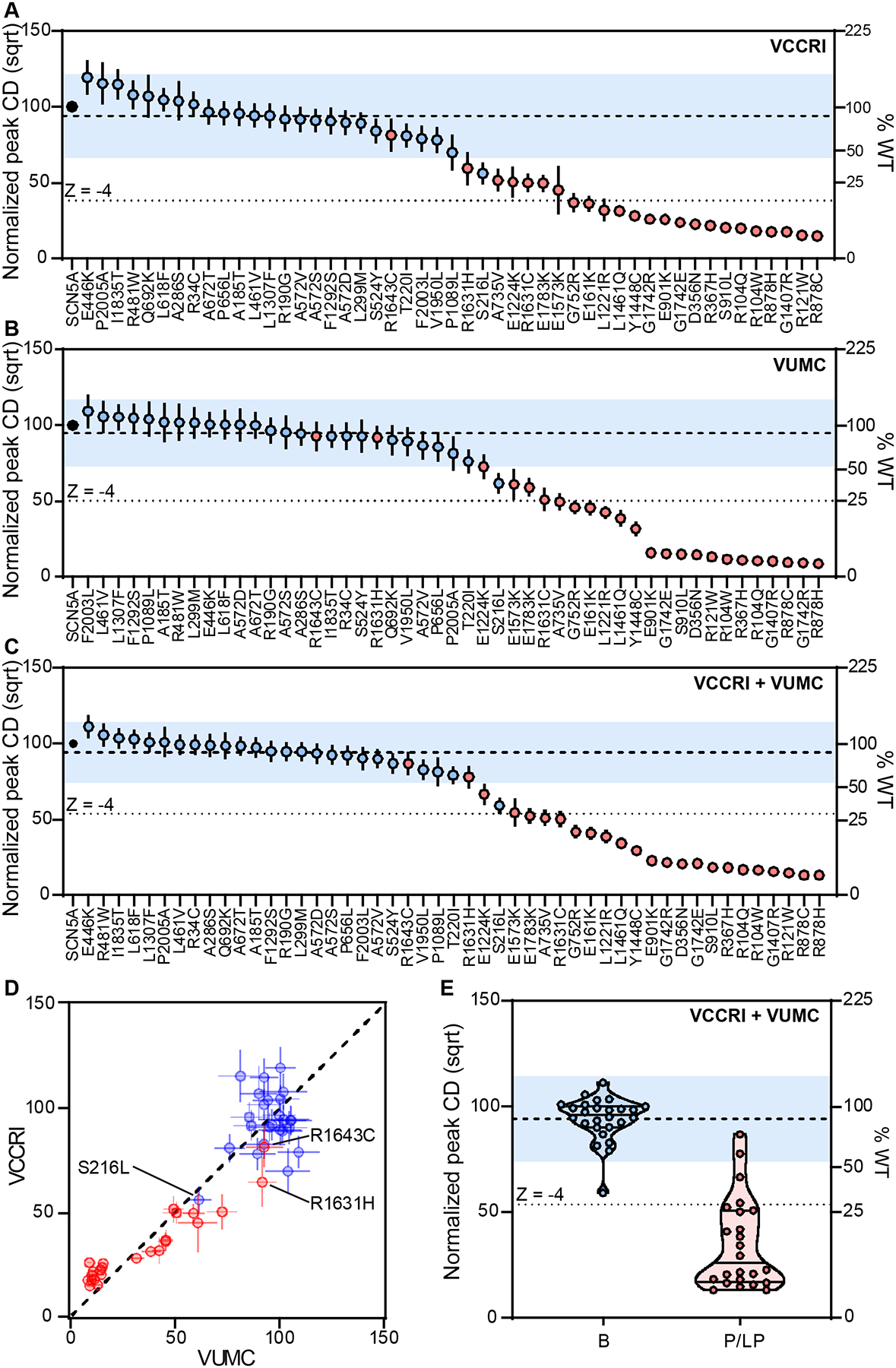
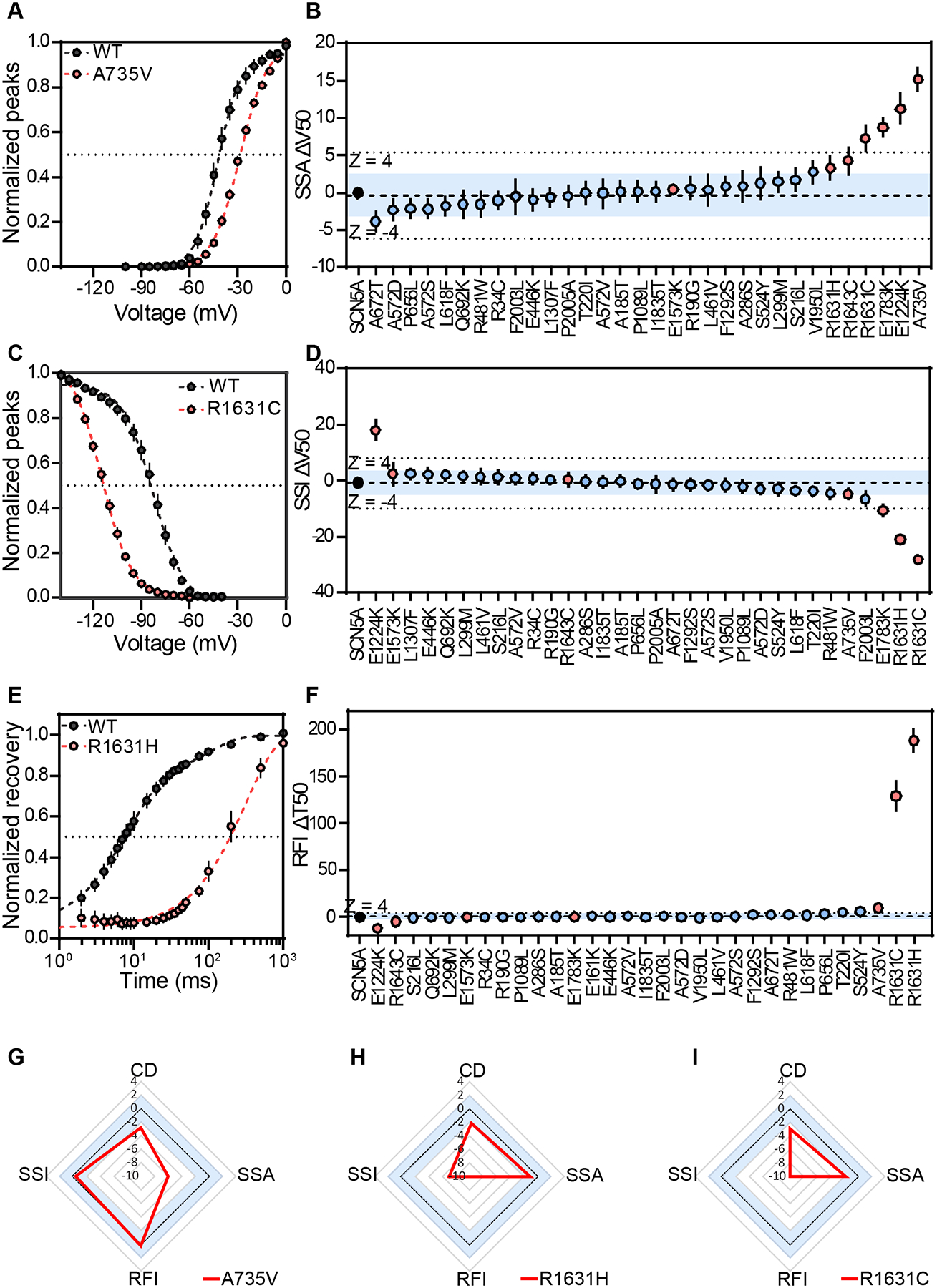
Results: Variant channel parameters generated independently at the 2 research sites showed strong correlations, including peak INa density (R2=0.86). The assay accurately distinguished benign controls (24/25 concordant variants) from pathogenic controls (23/24 concordant variants). Odds of pathogenicity values were 0.042 for normal function and 24.0 for abnormal function, corresponding to strong evidence for both American College of Medical Genetics and Genomics/Association for Molecular Pathology benign and pathogenic functional criteria (BS3 and PS3, respectively). Application of the assay to 4 clinical SCN5A variants of uncertain significance revealed loss-of-function for 3/4 variants, enabling reclassification to likely pathogenic.
Conclusions: This validated high-throughput assay provides clinical-grade functional evidence to aid the classification of current and future SCN5A-Brugada syndrome variants of uncertain significance.
Keywords: Brugada syndrome; arrhythmias, cardiac; genetic testing; patch-clamp techniques; voltage-gated sodium channels.
Conflict of interest statement
Dr Glazer is a consultant for BioMarin Inc Victoria Parikh is a scientific advisory board member (Lexeo Therapeutics), clinical advisor (Constantiam Biosciences), and consultant (BioMarin Inc, viz.ai). Dr Parikh also receives research support from BioMarin, Inc. The other authors report no conflicts.
Figures


Update of
-
Multi-site validation of a functional assay to adjudicate SCN5A Brugada Syndrome-associated variants.medRxiv [Preprint]. 2023 Dec 20:2023.12.19.23299592. doi: 10.1101/2023.12.19.23299592. medRxiv. 2023. Update in: Circ Genom Precis Med. 2024 Aug;17(4):e004569. doi: 10.1161/CIRCGEN.124.004569. PMID: 38196587 Free PMC article. Updated. Preprint.
References
-
- Brugada P, Brugada J. Right bundle branch block, persistent st segment elevation and sudden cardiac death: A distinct clinical and electrocardiographic syndrome. A multicenter report. J Am Coll Cardiol. 1992;20:1391–1396 - PubMed
-
- Cerrone M, Costa S, Delmar M. The genetics of brugada syndrome. Annu Rev Genomics Hum Genet. 2022 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
