

Extended-Infusion β-Lactam Therapy, Mortality, and Subsequent Antibiotic Resistance Among Hospitalized Adults With Gram-Negative Bloodstream Infections
- PMID: 38954416
- PMCID: PMC11220563
- DOI: 10.1001/jamanetworkopen.2024.18234
Extended-Infusion β-Lactam Therapy, Mortality, and Subsequent Antibiotic Resistance Among Hospitalized Adults With Gram-Negative Bloodstream Infections
Abstract
Importance: Current evidence is conflicting for associations of extended-infusion β-lactam (EI-BL) therapy with clinical outcomes.
Objective: To investigate the association of EI-BL therapy with survival, adverse events, and emergence of antibiotic resistance in adults with gram-negative bloodstream infections (GN-BSI).
Design, setting, and participants: This cohort study of consecutive adults with GN-BSI admitted to 24 United States hospitals between January 1, 2019, and December 31, 2019, receiving EI-BL were compared with adults with GN-BSI receiving the same agents as intermittent infusion β-lactam (II-BL; ≤1-hour infusions). Statistical analysis was performed from January to October 2023.
Exposures: EI-BL (ie, ≥3-hour infusion).
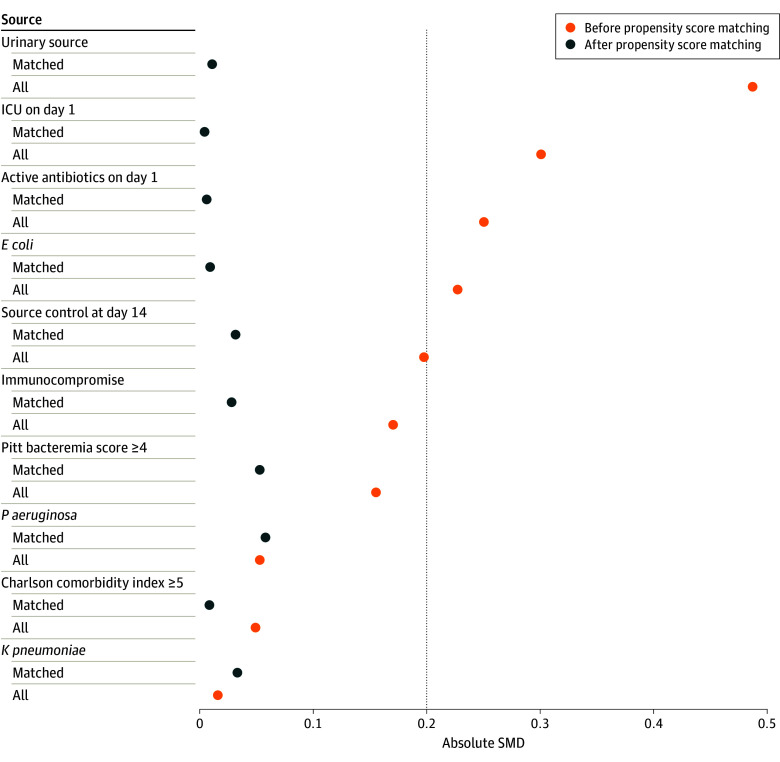
Main outcomes and measures: EI-BL and II-BL groups underwent 1:3 nearest-neighbor propensity score matching (PSM) without replacement. Multivariable regression was applied to the PSM cohort to investigate outcomes, all censored at day 90. The primary outcome was mortality; secondary outcomes included antibiotic adverse events and emergence of resistance (≥4-fold increase in the minimum inhibitory concentration of the β-lactam used to treat the index GN-BSI).
Results: Among the 4861 patients included, 2547 (52.4%) were male; and the median (IQR) age was 67 (55-77) years. There were 352 patients in the EI-BL 1:3 PSM group, and 1056 patients in the II-BL 1:3 PSM group. Among 1408 PSM patients, 373 (26.5%) died by day 90. The odds of mortality were lower in the EI-BL group (adjusted odds ratio [aOR], 0.71 [95% CI, 0.52-0.97]). In a stratified analysis, a survival benefit was only identified in patients with severe illness or elevated minimum inhibitory concentrations (ie, in the intermediate range for the antibiotic administered). There were increased odds of catheter complications (aOR, 3.14 [95% CI, 1.66-5.96]) and antibiotic discontinuation because of adverse events (eg, acute kidney injury, cytopenias, seizures) in the EI-BL group (aOR, 3.66 [95% CI, 1.68-7.95]). Emergence of resistance was similar in the EI-BL and II-BL groups at 2.9% vs 7.2%, respectively (P = .35).
Conclusions and relevance: In this cohort study of patients with GN-BSI, EI-BL therapy was associated with reduced mortality for patients with severe illness or those infected with nonsusceptible organisms; potential advantages in other groups remain unclear and need to be balanced with potential adverse events. The subsequent emergence of resistance warrants investigation in a larger cohort.
Conflict of interest statement
Figures
Comment in
-
Optimizing the Value of β-Lactam Antibiotics Through Extended Infusion.JAMA Netw Open. 2024 Jul 1;7(7):e2418196. doi: 10.1001/jamanetworkopen.2024.18196. JAMA Netw Open. 2024. PMID: 38954420 No abstract available.
Similar articles
-
Extended Infusion of β-Lactams for Bloodstream Infection in Patients With Liver Cirrhosis: An Observational Multicenter Study.Clin Infect Dis. 2019 Oct 30;69(10):1731-1739. doi: 10.1093/cid/ciz032. Clin Infect Dis. 2019. PMID: 30649218
-
Loading dose plus continuous/extended infusion versus intermittent bolus of β-lactams for the treatment of Gram-negative bacteria bloodstream infections: a propensity score-adjusted retrospective cohort study.J Antimicrob Chemother. 2023 Sep 5;78(9):2175-2184. doi: 10.1093/jac/dkad215. J Antimicrob Chemother. 2023. PMID: 37428015
-
Risk factors for treatment failure in patients receiving β-lactam/β-lactamase inhibitor combinations for Enterobacteriaceae bloodstream infection: A retrospective, single-centre, cohort study.Int J Antimicrob Agents. 2019 May;53(5):574-581. doi: 10.1016/j.ijantimicag.2019.01.005. Epub 2019 Jan 9. Int J Antimicrob Agents. 2019. PMID: 30639527
-
Evaluation of studies on extended versus standard infusion of beta-lactam antibiotics.Am J Health Syst Pharm. 2019 Sep 3;76(18):1383-1394. doi: 10.1093/ajhp/zxz154. Am J Health Syst Pharm. 2019. PMID: 31505562 Review.
-
Beta-lactam/beta-lactamase inhibitors versus carbapenem for bloodstream infections due to extended-spectrum beta-lactamase-producing Enterobacteriaceae: systematic review and meta-analysis.Int J Antimicrob Agents. 2018 Nov;52(5):554-570. doi: 10.1016/j.ijantimicag.2018.07.021. Epub 2018 Aug 3. Int J Antimicrob Agents. 2018. PMID: 30081138
Cited by
-
Therapeutic Drug Monitoring of Antimicrobial Drugs in Children with Cancer: A New Tool for Personalized Medicine.Paediatr Drugs. 2025 Jan;27(1):41-56. doi: 10.1007/s40272-024-00663-5. Epub 2024 Nov 6. Paediatr Drugs. 2025. PMID: 39503988 Review.
-
[Empirical antibiotic therapy in life-threatening infections-current concepts and controversies].Anaesthesiologie. 2025 Aug;74(8):476-488. doi: 10.1007/s00101-025-01531-8. Epub 2025 May 15. Anaesthesiologie. 2025. PMID: 40372450 German.
-
How to approach a patient hospitalized for pneumonia who is not responding to treatment?Intensive Care Med. 2025 May;51(5):893-903. doi: 10.1007/s00134-025-07903-3. Epub 2025 May 24. Intensive Care Med. 2025. PMID: 40411623 Free PMC article. Review.
-
The Definition, Prevalence, and Risk Factors of Augmented Renal Clearance in Adult Patients on Antimicrobial Therapy: A Scoping Review.Infect Dis Clin Microbiol. 2025 Jun 26;7(2):123-132. doi: 10.36519/idcm.2025.504. eCollection 2025 Jun. Infect Dis Clin Microbiol. 2025. PMID: 40657020 Free PMC article.
-
Population pharmacokinetics and dose optimization of ceftazidime in critically ill children.Front Pharmacol. 2024 Nov 27;15:1470350. doi: 10.3389/fphar.2024.1470350. eCollection 2024. Front Pharmacol. 2024. PMID: 39664522 Free PMC article.
References
-
- Roberts JA, Kirkpatrick CMJ, Roberts MS, Dalley AJ, Lipman J. First-dose and steady-state population pharmacokinetics and pharmacodynamics of piperacillin by continuous or intermittent dosing in critically ill patients with sepsis. Int J Antimicrob Agents. 2010;35(2):156-163. doi:10.1016/j.ijantimicag.2009.10.008 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
