

Long-term outcomes of extensive thoracoabdominal aortic aneurysm repair utilizing normothermic iliac perfusion: a retrospective cohort study with 10-year single-center experience
- PMID: 38954673
- PMCID: PMC11745653
- DOI: 10.1097/JS9.0000000000001858
Long-term outcomes of extensive thoracoabdominal aortic aneurysm repair utilizing normothermic iliac perfusion: a retrospective cohort study with 10-year single-center experience
Abstract
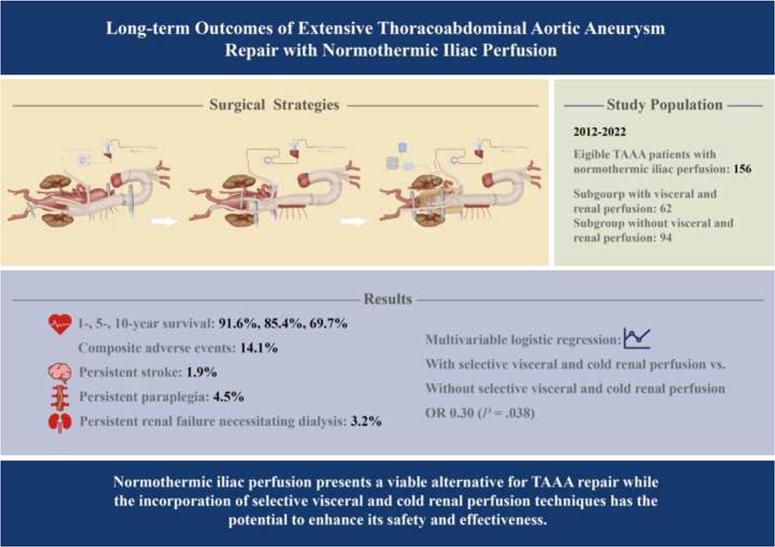
Background: Normothermic iliac perfusion has been increasingly utilized for thoracoabdominal aortic aneurysm repair; however, the long-term outcomes in large samples are lacking. This study was designed to assess the perioperative and long-term results of thoracoabdominal aortic repair using normothermic iliac perfusion.
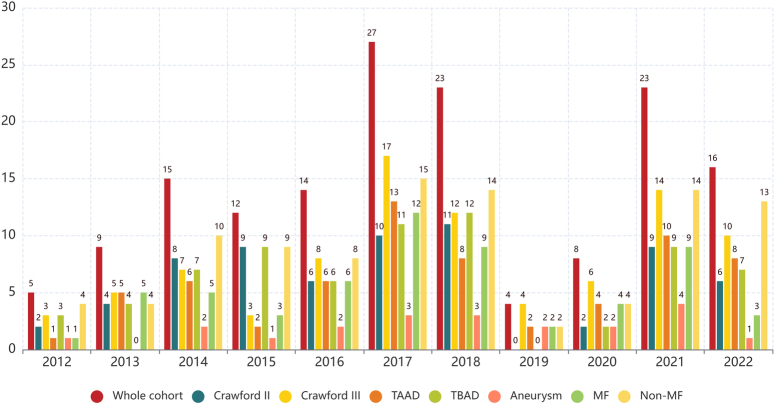
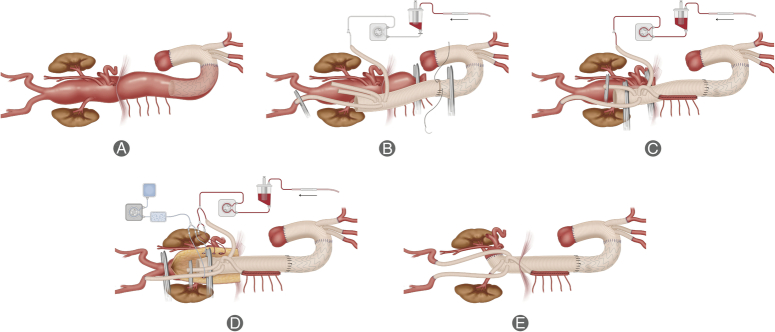
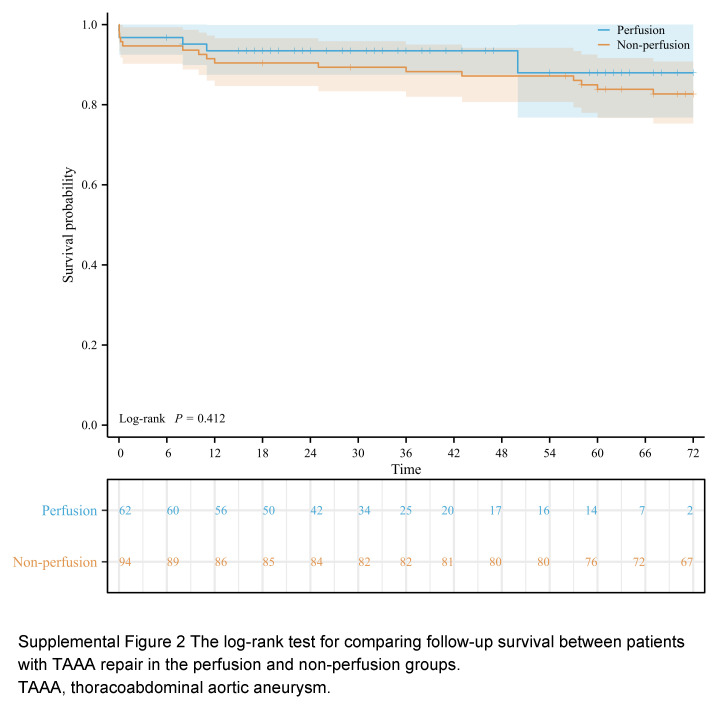
Methods: The authors retrospectively analyzed 156 patients having Crawford extent II or III thoracoabdominal aortic aneurysm replacement with normothermic iliac perfusion from 2012 to 2022. Primary endpoints were composite adverse events and long-term survival, which encompassed 30-day mortality, persistent stroke, persistent paraplegia, and acute renal failure needing continuous dialysis. The cohort was divided into two subgroups based on the use of selective visceral and cold renal perfusion techniques.
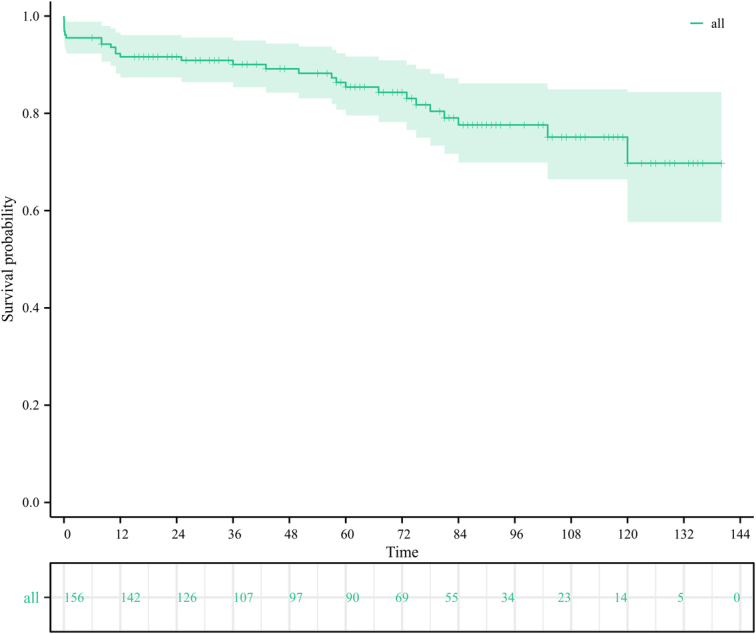
Results: The combined adverse event rate was 14.1%. Specific rates were: 30-day mortality (4.5%), persistent stroke (1.9%), persistent paraplegia (4.5%), and renal failure requiring persistent dialysis (3.2%). The median follow-up time was 67 months. Overall survival rates at 1, 3, 5, 7, and 10 years were 91.6, 90.0, 85.4, 77.6, and 69.7%, respectively. Subgroup analysis showed the visceral and renal perfusion group had a significantly reduced adverse event incidence compared to the nonperfusion group (6.5 vs. 19.1%, P =0.026). Multivariable logistic regression analysis confirmed selective visceral and cold renal perfusion techniques as protective factors against postoperative adverse events (OR 0.30, 95% CI: 0.09-0.94; P =0.038). Multivariable Cox regression analysis identified age ≥50 years (HR 2.63, 95% CI: 1.10-6.27; P =0.029) and NYHA grade ≥III (HR: 3.20, 95% CI: 1.04-9.87; P =0.043) as independent risk factors predicting overall survival.
Conclusions: Normothermic iliac perfusion is a feasible option for thoracoabdominal aortic repair with cost benefits and simpler management, and selective visceral and cold renal perfusion techniques may further improve its safety and effectiveness. However, enhanced vigilance and meticulous care are essential, particularly for elderly patients and those with cardiac insufficiency.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare that they have no financial conflict of interest with regard to the content of this report.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures
Similar articles
-
Comparative analysis of long-term outcomes in thoracoabdominal aortic aneurysm repair between Marfan syndrome patients and non-Marfan syndrome patients.J Thorac Cardiovasc Surg. 2025 Jul;170(1):146-155.e1. doi: 10.1016/j.jtcvs.2024.08.018. Epub 2024 Aug 22. J Thorac Cardiovasc Surg. 2025. PMID: 39178942
-
Spinal cord protection by normothermic artery bypass and visceral-anastomosis-first strategy in thoracoabdominal aortic aneurysm repair.BMC Cardiovasc Disord. 2025 Apr 7;25(1):261. doi: 10.1186/s12872-025-04710-y. BMC Cardiovasc Disord. 2025. PMID: 40189531 Free PMC article.
-
Outcomes of 3309 thoracoabdominal aortic aneurysm repairs.J Thorac Cardiovasc Surg. 2016 May;151(5):1323-37. doi: 10.1016/j.jtcvs.2015.12.050. Epub 2016 Jan 14. J Thorac Cardiovasc Surg. 2016. PMID: 26898979
-
Comparison of single- and multistage strategies during fenestrated-branched endovascular aortic repair of thoracoabdominal aortic aneurysms.J Vasc Surg. 2023 Jun;77(6):1588-1597.e4. doi: 10.1016/j.jvs.2023.01.188. Epub 2023 Jan 31. J Vasc Surg. 2023. PMID: 36731757 Review.
-
Systematic review and meta-analysis of published studies on endovascular repair of thoracoabdominal aortic aneurysms with the t-Branch off-the-shelf multibranched endograft.J Vasc Surg. 2020 Aug;72(2):716-725.e1. doi: 10.1016/j.jvs.2020.01.049. Epub 2020 Apr 1. J Vasc Surg. 2020. PMID: 32247700
References
-
- Kouchoukos NT, Daily BB, Rokkas CK, et al. . Hypothermic bypass and circulatory arrest for operations on the descending thoracic and thoracoabdominal aorta. Ann Thorac Surg 1995;60:67–76. - PubMed
-
- Kouchoukos NT, Masetti P, Castner CF. Use of presewn multiple branched graft in thoracoabdominal aortic aneurysm repair. J Am Coll Surg 2005;201:646–649. - PubMed
-
- Iguro Y, Yotsumoto G, Ishizaki N, et al. . Endovascular stent-graft repair for thoracoabdominal aneurysm after reconstruction of the superior mesenteric and celiac arteries. J Thorac Cardiovasc Surg 2003;125:956–958. - PubMed
-
- Rimmer J, Wolfe JH. Type III thoracoabdominal aortic aneurysm repair: a combined surgical and endovascular approach. Eur J Vasc Endovasc Surg 2003;26:677–679. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
