

Risk of emergency hospital admission related to adverse events after antibiotic treatment in adults with a common infection: impact of COVID-19 and derivation and validation of risk prediction models
- PMID: 38956603
- PMCID: PMC11220965
- DOI: 10.1186/s12916-024-03480-2
Risk of emergency hospital admission related to adverse events after antibiotic treatment in adults with a common infection: impact of COVID-19 and derivation and validation of risk prediction models
Abstract
Background: With the global challenge of antimicrobial resistance intensified during the COVID-19 pandemic, evaluating adverse events (AEs) post-antibiotic treatment for common infections is crucial. This study aims to examines the changes in incidence rates of AEs during the COVID-19 pandemic and predict AE risk following antibiotic prescriptions for common infections, considering their previous antibiotic exposure and other long-term clinical conditions.
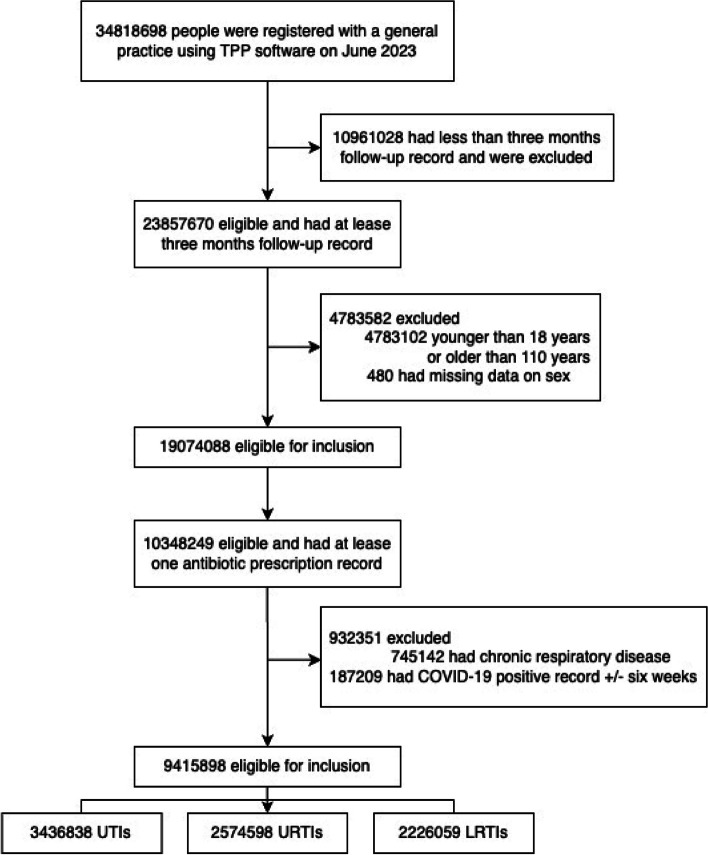
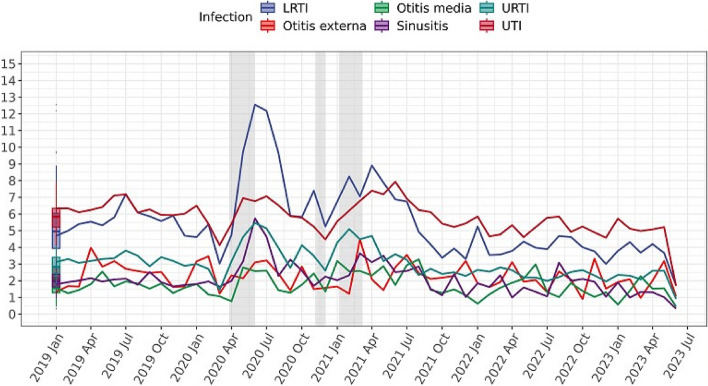
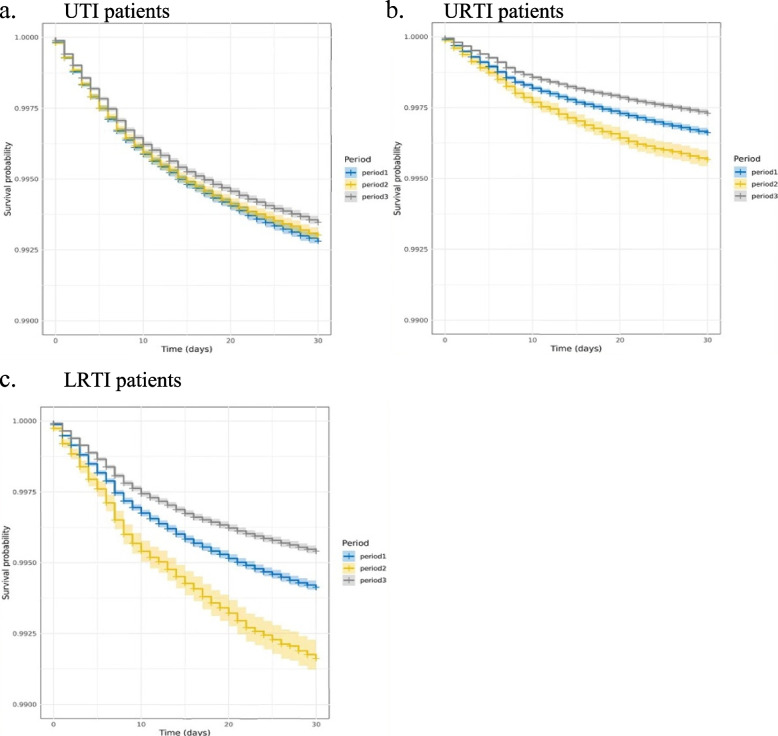
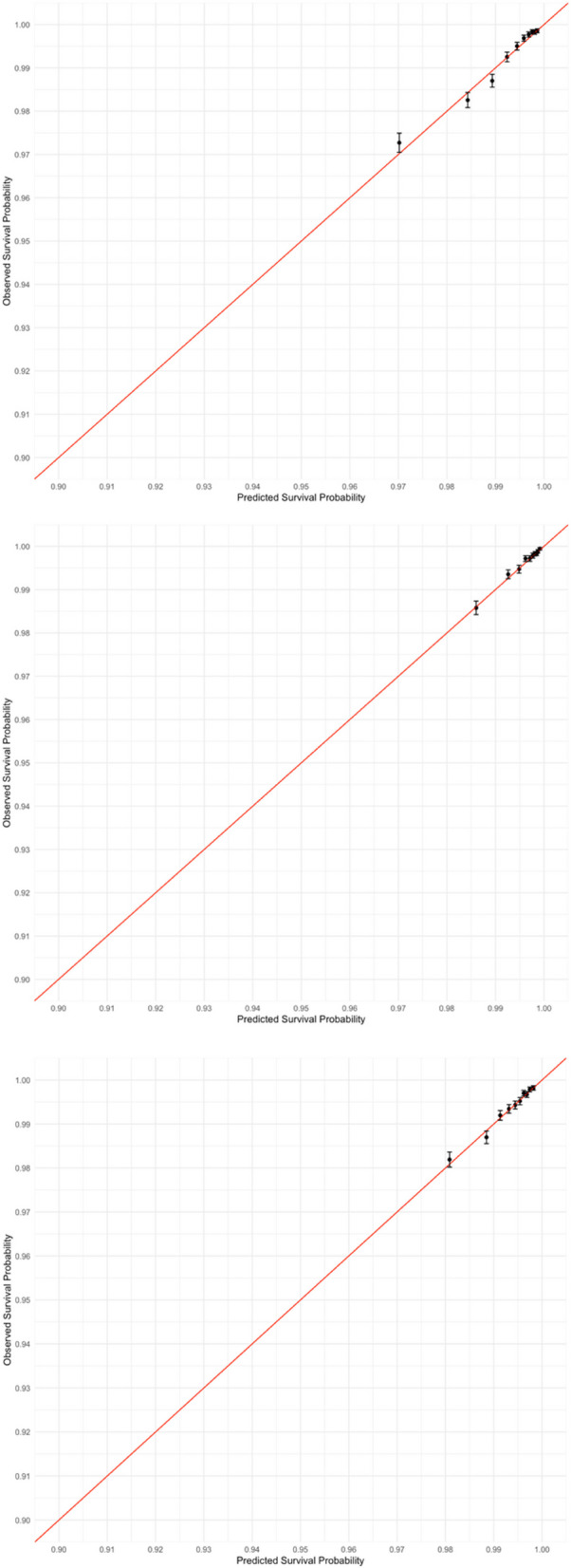
Methods: With the approval of NHS England, we used OpenSAFELY platform and analysed electronic health records from patients aged 18-110, prescribed antibiotics for urinary tract infection (UTI), lower respiratory tract infections (LRTI), upper respiratory tract infections (URTI), sinusitis, otitis externa, and otitis media between January 2019 and June 2023. We evaluated the temporal trends in the incidence rate of AEs for each infection, analysing monthly changes over time. The survival probability of emergency AE hospitalisation was estimated in each COVID-19 period (period 1: 1 January 2019 to 25 March 2020, period 2: 26 March 2020 to 8 March 2021, period 3: 9 March 2021 to 30 June 2023) using the Kaplan-Meier approach. Prognostic models, using Cox proportional hazards regression, were developed and validated to predict AE risk within 30 days post-prescription using the records in Period 1.
Results: Out of 9.4 million patients who received antibiotics, 0.6% of UTI, 0.3% of URTI, and 0.5% of LRTI patients experienced AEs. UTI and LRTI patients demonstrated a higher risk of AEs, with a noted increase in AE incidence during the COVID-19 pandemic. Higher comorbidity and recent antibiotic use emerged as significant AE predictors. The developed models exhibited good calibration and discrimination, especially for UTIs and LRTIs, with a C-statistic above 0.70.
Conclusions: The study reveals a variable incidence of AEs post-antibiotic treatment for common infections, with UTI and LRTI patients facing higher risks. AE risks varied between infections and COVID-19 periods. These findings underscore the necessity for cautious antibiotic prescribing and call for further exploration into the intricate dynamics between antibiotic use, AEs, and the pandemic.
Keywords: Adverse event; Antibiotics; COVID-19 pandemic; Common infection.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- English surveillance programme for antimicrobial utilisation and resistance (ESPAUR) report - GOV.UK. Available from: https://www.gov.uk/government/publications/english-surveillance-programm.... Cited 2023 Aug 30.
-
- English surveillance programme for antimicrobial utilisation and resistance (ESPAUR) report - GOV.UK. Available from: https://www.gov.uk/government/publications/english-surveillance-programm.... Cited 2022 Nov 29.
-
- Zhong X, Pate A, Yang YT, Fahmi A, Ashcroft DM, Goldacre B, et al. The impact of COVID-19 on antibiotic prescribing in primary care in England: evaluation and risk prediction of appropriateness of type and repeat prescribing. J Infect. 2023;87(1):1–11. doi: 10.1016/j.jinf.2023.05.010. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
