

Effects of ganaxolone on non-seizure outcomes in CDKL5 Deficiency Disorder: Double-blind placebo-controlled randomized trial
- PMID: 38959712
- PMCID: PMC11283350
- DOI: 10.1016/j.ejpn.2024.06.005
Effects of ganaxolone on non-seizure outcomes in CDKL5 Deficiency Disorder: Double-blind placebo-controlled randomized trial
Abstract
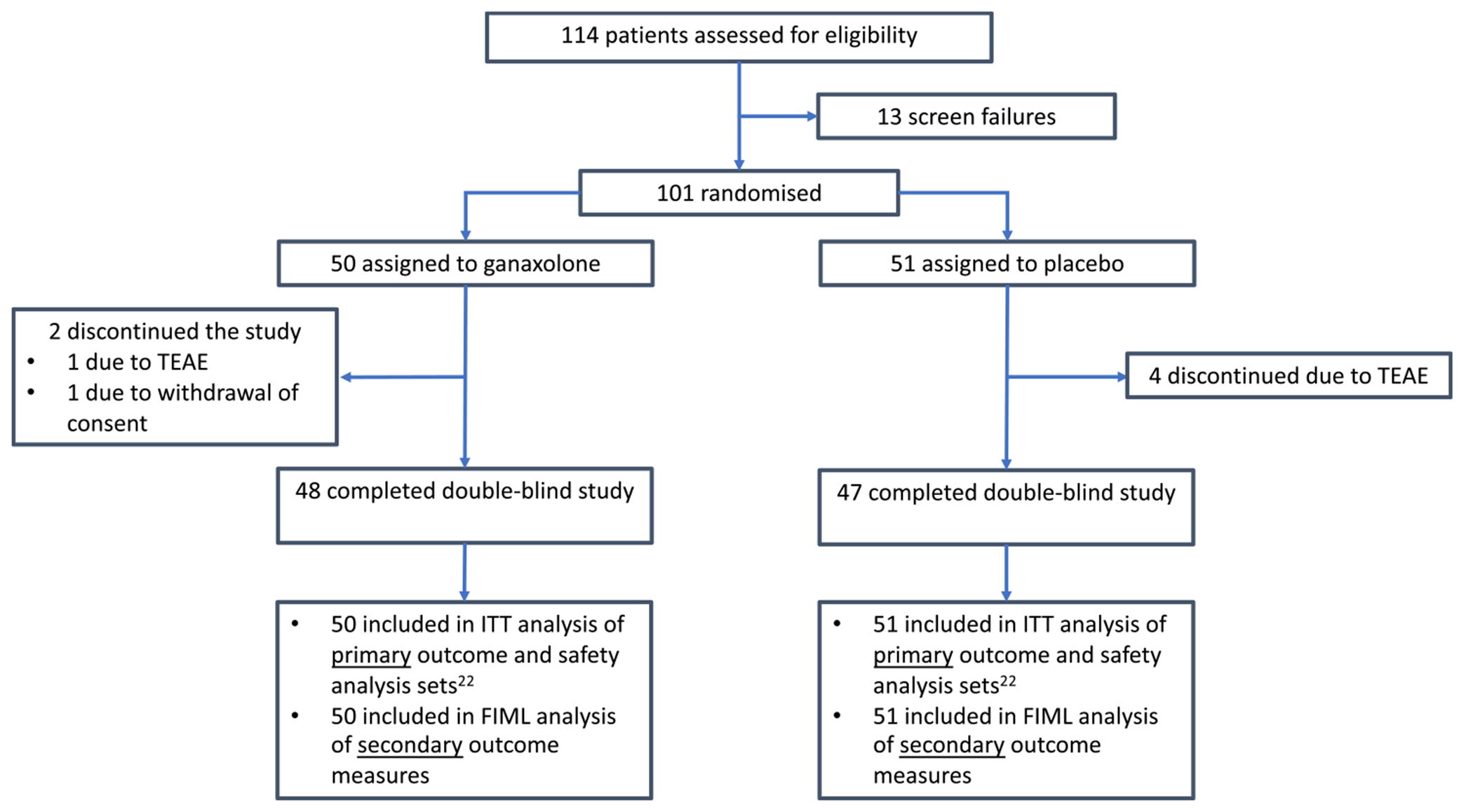
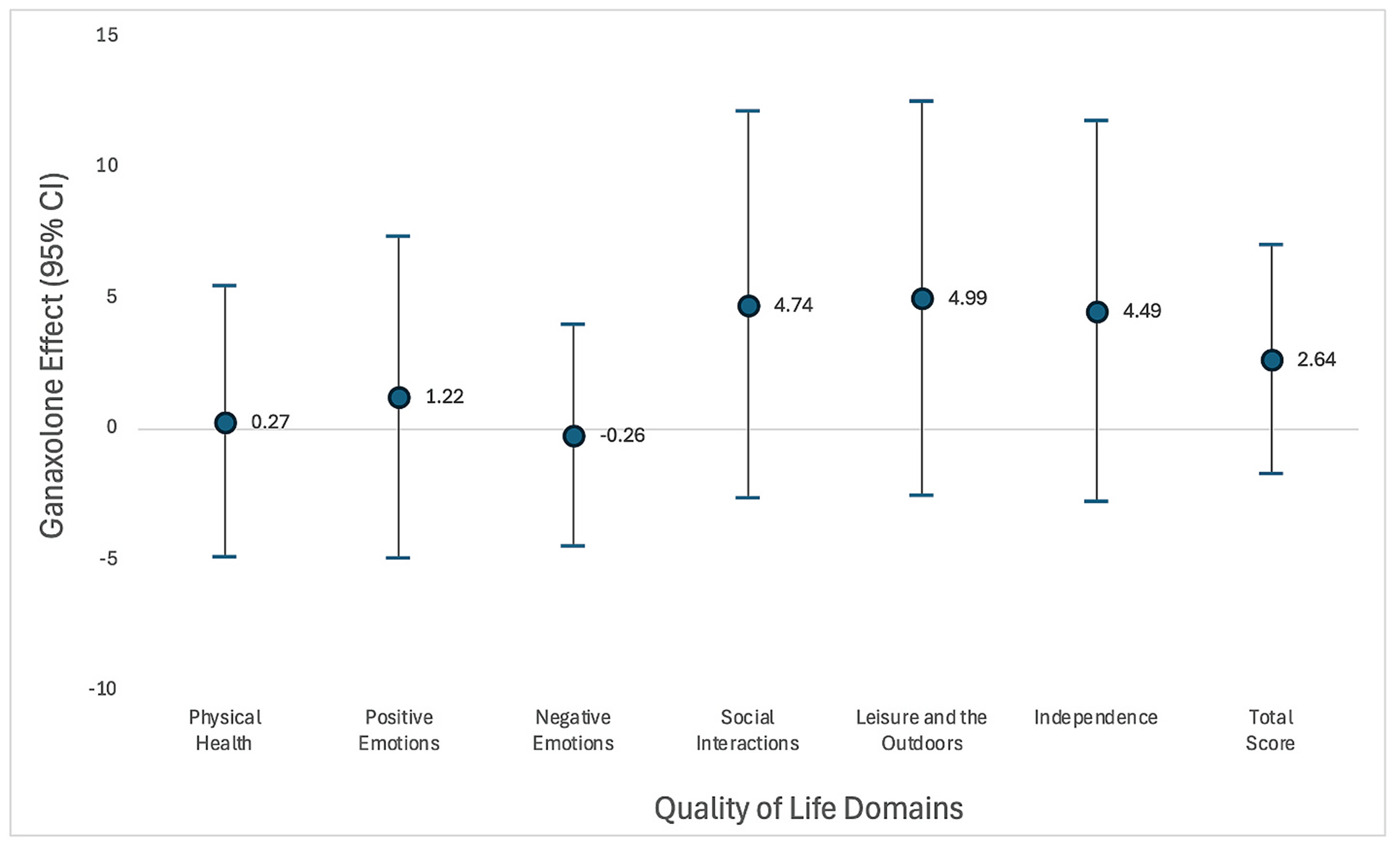
CDKL5 deficiency disorder (CDD) is a rare developmental and epileptic encephalopathy. Ganaxolone, a neuroactive steroid, reduces the frequency of major motor seizures in children with CDD. This analysis explored the effect of ganaxolone on non-seizure outcomes. Children (2-19 years) with genetically confirmed CDD and ≥ 16 major motor seizures per month were enrolled in a double-blind randomized placebo-controlled trial. Ganaxolone or placebo was administered three times daily for 17 weeks. Behaviour was measured with the Anxiety, Depression and Mood Scale (ADAMS), daytime sleepiness with the Child Health Sleep Questionnaire, and quality of life with the Quality of Life Inventory-Disability (QI-Disability) scale. Scores were compared using ANOVA, adjusted for age, sex, number of anti-seizure mediations, baseline 28-day major motor seizure frequency, baseline developmental skills, and behaviour, sleep or quality of life scores. 101 children with CDD (39 clinical sites, 8 countries) were randomized. Median (IQR) age was 6 (3-10) years, 79.2 % were female, and 50 received ganaxolone. After 17 weeks of treatment, Manic/Hyperactive scores (mean difference 1.27, 95%CI -2.38,-0.16) and Compulsive Behaviour scores (mean difference 0.58, 95%CI -1.14,-0.01) were lower (improved) in the ganaxolone group compared with the placebo group. Daytime sleepiness scores were similar between groups. The total change in QOL score for children in the ganaxolone group was 2.6 points (95%CI -1.74,7.02) higher (improved) than in the placebo group but without statistical significance. Along with better seizure control, children who received ganaxolone had improved behavioural scores in select domains compared to placebo.
Keywords: Anti-Seizure medication; CDKL5 deficiency disorder; Epilepsy; Patient-reported outcomes.
Copyright © 2024 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of competing interest Jenny Downs: Consultancy for Marinus, Ultragenyx, Orion and Taysha; Clinical Trials with Anavex; All remuneration has been made to her department. Peter Jacoby: No conflicts of interest to report. Nicola Specchio: served on scientific advisory boards for GW Pharma, BioMarin, Arvelle, Marinus and Takeda; has received speaker honoraria from Eisai, Biomarin, Livanova, Sanofi; has served as an investigator for Zogenix, Marinus, Biomarin, UCB, Roche. Helen Cross: acted as an investigator for studies with GW Pharma, Ovid Therapeutics, Zogenix, Vitaflo, Marinius and Stoke Therapeutics. She has been a speaker and on advisory boards for GW Pharma, Zogenix, UCB and Nutricia; all remuneration has been paid to her department. She holds an endowed chair at UCL Great Ormond Street Institute of Child Health; she holds grants from NIHR, EPSRC, GOSH Charity, ERUK, the Waterloo Foundation and the National Institute of Health Research (NIHR) Biomedical Research Centre at Great Ormond Street Hospital. Sam Amin: SA has received funding from GW Pharmaceuticals, Novartis, PTC Therapeutics, Boston Scientific, Nutricia, UCB, BioMarin, LivaNova, Medtronic, Desitin, Ipsen, Orion, CDKL5 UK, TSA and the National Institute for Health Research. Nadia Bahi-Buisson: Consultancy for Marinus, Orion. Rajsekar Rajaraman: Consultancy for Marinus, Ultragenyx, Zogenix. Bernard Suter: Consultancy for Neurogene and Taysha; all remuneration has been paid to his department. Acted as investigator for clinical trials with Acadia, Marinus and Newron. Orrin Devinsky: Orrin Devinsky has equity and/or compensation from the following companies: Tilray, Receptor Life Sciences, Qstate Biosciences, Hitch Biosciences, Tevard Biosciences, Regel Biosciences, Script Biosciences, Actio Biosciences, Empatica, SilverSpike, and California Cannabis Enterprises (CCE). He has received consulting fees from Zogenix, Ultragenyx, BridgeBio, GeneMedicine and Marinus. He holds patents for the use of cannabidiol in treating neurological disorders and others in molecular biology. He is the managing partner of PhiFund Ventures. Alex Aimetti: Employee of Marinus Pharmaceuticals. Gregory Busse: Previously an employee of Marinus Pharmaceuticals. Heather Olson: Dr. Olson received consulting fees from Takeda Pharmaceuticals and Zogenix regarding clinical trial design, Ovid Therapeutics regarding clinical trial results, Marinus Pharmaceuticals regarding CDKL5 Deficiency Disorder, and has done consulting for the FOXG1 Research Foundation. Scott Demarest: Consulted for Biomarin, Neurogene, Marinus, Tysha, Ultragenyx, Zogenix and Ovid Therapeutics. He has funding from project 8P and Mila's Miracle Foundation. He also serves on the advisory board for the non-profit foundations SLC6A1 Connect, Project 8P, Ring14 USA and FamilieSCN2A. Tim Benke: Consultancy for Acadia, CUREGRI, GRINtherapeutics, GW, IRSF, Marinus, Neurogene, Taysha, Ultragenyx and Zogenix; Clinical Trials with Acadia, RSRT and GW; all remuneration has been made to his department. Elia Pestana-Knight: Scientific Advisory Board, Marinus Pharmaceuticals.
Figures

References
-
- Lindy AS, Stosser MB, Butler E, et al., Diagnostic outcomes for genetic testing of 70 genes in 8565 patients with epilepsy and neurodevelopmental disorders, Epilepsia 59 (5) (2018) 1062–1071. - PubMed
-
- Zuberi SM, Wirrell E, Yozawitz E, et al., ILAE classification and definition of epilepsy syndromes with onset in neonates and infants: position statement by the ILAE Task Force on Nosology and Definitions, Epilepsia 63 (6) (2022) 1349–1397. - PubMed
