

Infection and the microbiome in bronchiectasis
- PMID: 38960615
- PMCID: PMC11220623
- DOI: 10.1183/16000617.0038-2024
Infection and the microbiome in bronchiectasis
Abstract
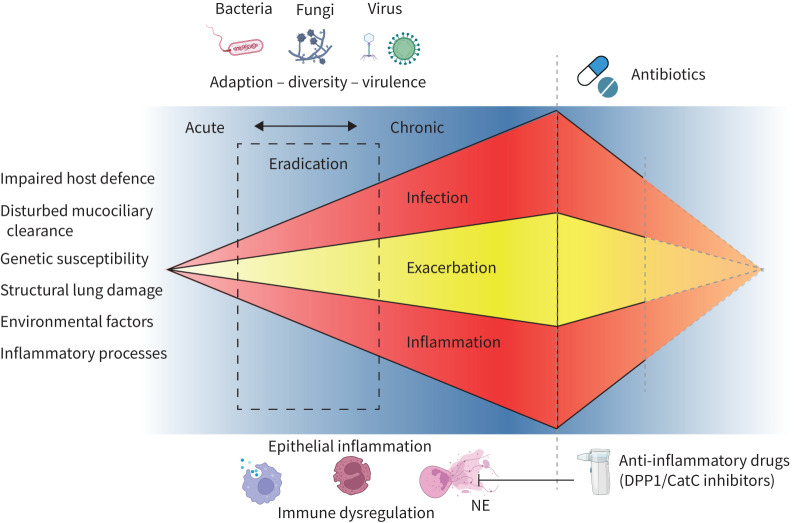
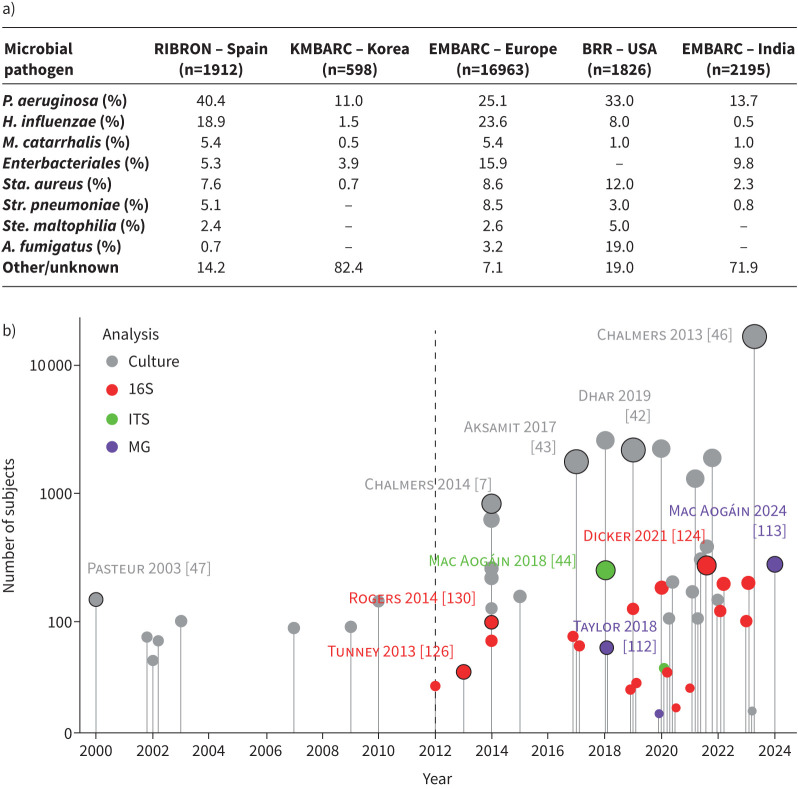
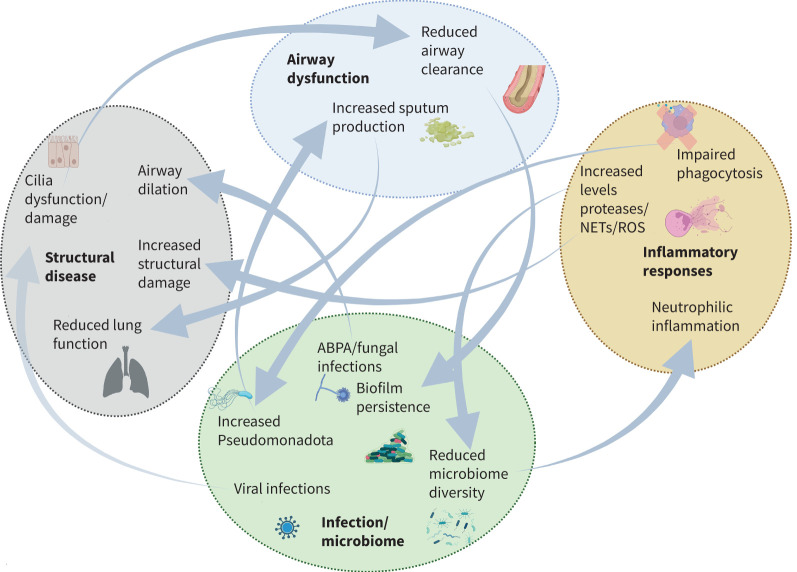
Bronchiectasis is marked by bronchial dilatation, recurrent infections and significant morbidity, underpinned by a complex interplay between microbial dysbiosis and immune dysregulation. The identification of distinct endophenotypes have refined our understanding of its pathogenesis, including its heterogeneous disease mechanisms that influence treatment and prognosis responses. Next-generation sequencing (NGS) has revolutionised the way we view airway microbiology, allowing insights into the "unculturable". Understanding the bronchiectasis microbiome through targeted amplicon sequencing and/or shotgun metagenomics has provided key information on the interplay of the microbiome and host immunity, a central feature of disease progression. The rapid increase in translational and clinical studies in bronchiectasis now provides scope for the application of precision medicine and a better understanding of the efficacy of interventions aimed at restoring microbial balance and/or modulating immune responses. Holistic integration of these insights is driving an evolving paradigm shift in our understanding of bronchiectasis, which includes the critical role of the microbiome and its unique interplay with clinical, inflammatory, immunological and metabolic factors. Here, we review the current state of infection and the microbiome in bronchiectasis and provide views on the future directions in this field.
Copyright ©The authors 2024.
Conflict of interest statement
Conflict of interest: S.H. Chotirmall serves on advisory boards for CSL Behring, Pneumagen Ltd and Boehringer Ingelheim, has received lecture fees from AstraZeneca and Chiesi Farmaceutici and has served on data safety and monitoring boards (DSMBs) for Inovio Pharmaceuticals Ltd and Imam Abdulrahman Bin Faisal University. All other authors have no conflicts to disclose.
Figures
Comment in
- doi: 10.1183/16000617.0124-2024
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources