

Diffuse-Type Histology Is Prognostic for All Siewert Types of Gastroesophageal Adenocarcinoma
- PMID: 38960886
- PMCID: PMC11224723
- DOI: 10.5230/jgc.2024.24.e20
Diffuse-Type Histology Is Prognostic for All Siewert Types of Gastroesophageal Adenocarcinoma
Abstract
Purpose: The optimal treatment for gastroesophageal junction adenocarcinoma (GEJA) remains controversial. We evaluated the treatment patterns and outcomes of patients with locally advanced GEJA according to the histological type.
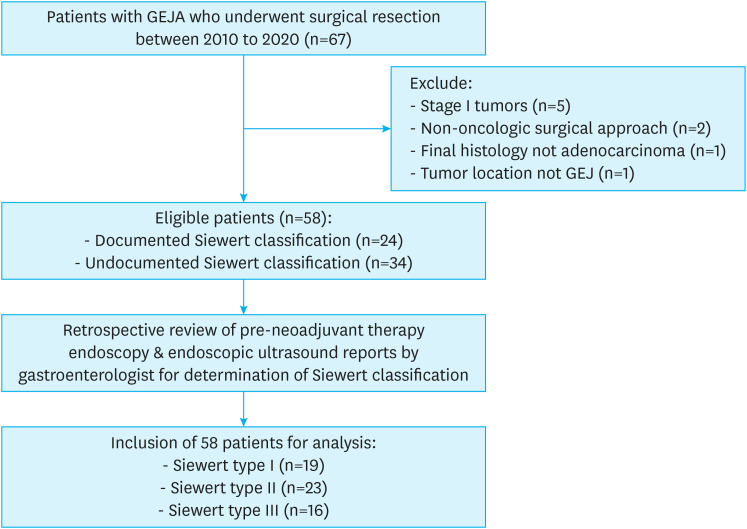
Materials and methods: We conducted a single-institution retrospective cohort study of patients with locally advanced GEJA who underwent curative-intent surgical resection between 2010 and 2020. Perioperative therapies as well as clinicopathologic, surgical, and survival data were collected. The results of endoscopy and histopathological examinations were assessed for Siewert and Lauren classifications.
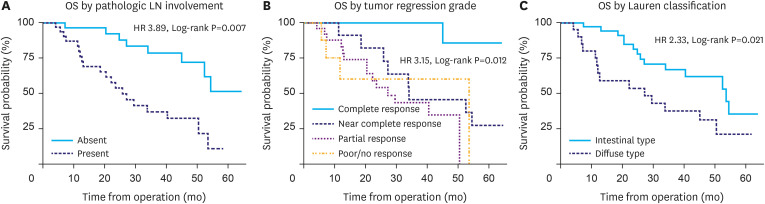
Results: Among the 58 patients included in this study, 44 (76%) were clinical stage III, and all received neoadjuvant therapy (72% chemoradiation, 41% chemotherapy, 14% both chemoradiation and chemotherapy). Tumor locations were evenly distributed by Siewert Classification (33% Siewert-I, 40% Siewert-II, and 28% Siewert-III). Esophagogastrectomy (EG) was performed for 47 (81%) patients and total gastrectomy (TG) for 11 (19%) patients. All TG patients received D2 lymphadenectomy compared to 10 (21%) EG patients. Histopathological examination showed the presence of 64% intestinal-type and 36% diffuse-type histology. The frequencies of diffuse-type histology were similar among Siewert groups (37% Siewert-I, 36% Siewert-II, and 33% Siewert-III). Regardless of Siewert type and compared to intestinal-type, diffuse histology was associated with increased intraabdominal recurrence rates (P=0.03) and decreased overall survival (hazard ratio, 2.33; P=0.02). With a median follow-up of 31.2 months, 29 (50%) patients had a recurrence, and the median overall survival was 50.5 months.
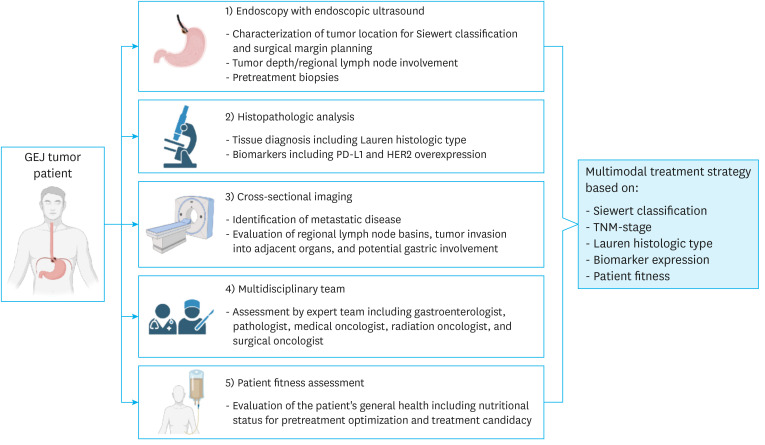
Conclusions: Present in equal proportions among Siewert types of esophageal and gastric cancer, a diffuse-type histology was associated with high intraabdominal recurrence rates and poor survival. Histopathological evaluation should be considered in addition to anatomic location in the determination of multimodal GEJA treatment strategies.
Keywords: Esophageal cancer; Esophagogastric junction adenocarcinoma; Gastric cancer; Histology evaluation; Siewert-Stein classification.
Copyright © 2024. Korean Gastric Cancer Association.
Conflict of interest statement
Dr. Woo is a scientific consultant for Johnson & Johnson Ethicon and serves on the advisory board of Imugene. Dr. Fong is a scientific consultant for Medtronics, Covidien, Xdemics, Vergent Biosciences, Eureka Biologics, and Imugene; receives royalties from Merck and Imugene; has a research study agreement with Imugene; a member of Dr. Fong's family is President and CEO of XDemics. There are no disclosures for the remaining authors.
Figures
References
-
- Bartel M, Brahmbhatt B, Bhurwal A. Incidence of gastroesophageal junction cancer continues to rise: analysis of Surveillance, Epidemiology, and End Results (SEER) database. J Clin Oncol. 2019;37:40.
-
- Shapiro J, van Lanschot JJB, Hulshof MCCM, van Hagen P, van Berge Henegouwen MI, Wijnhoven BPL, et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): long-term results of a randomised controlled trial. Lancet Oncol. 2015;16:1090–1098. - PubMed
-
- Al-Batran SE, Homann N, Pauligk C, Goetze TO, Meiler J, Kasper S, et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet. 2019;393:1948–1957. - PubMed
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
