

Ensemble learning for fetal ultrasound and maternal-fetal data to predict mode of delivery after labor induction
- PMID: 38961231
- PMCID: PMC11222528
- DOI: 10.1038/s41598-024-65394-6
Ensemble learning for fetal ultrasound and maternal-fetal data to predict mode of delivery after labor induction
Erratum in
-
Author Correction: Ensemble learning for fetal ultrasound and maternal-fetal data to predict mode of delivery after labor induction.Sci Rep. 2024 Aug 6;14(1):18237. doi: 10.1038/s41598-024-69015-0. Sci Rep. 2024. PMID: 39107457 Free PMC article. No abstract available.
Abstract
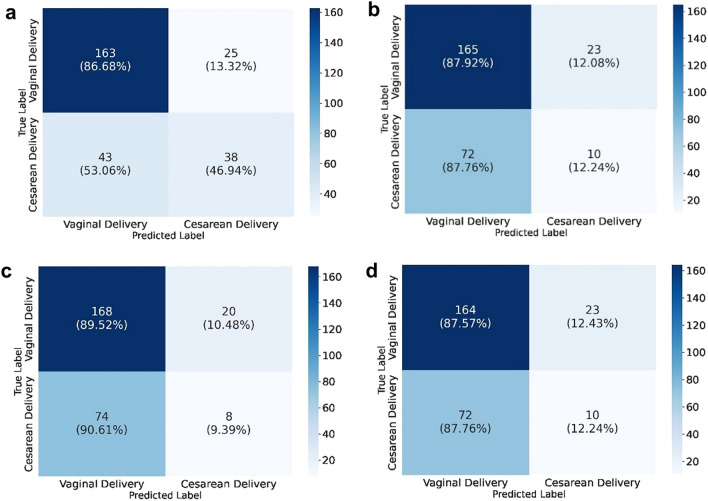
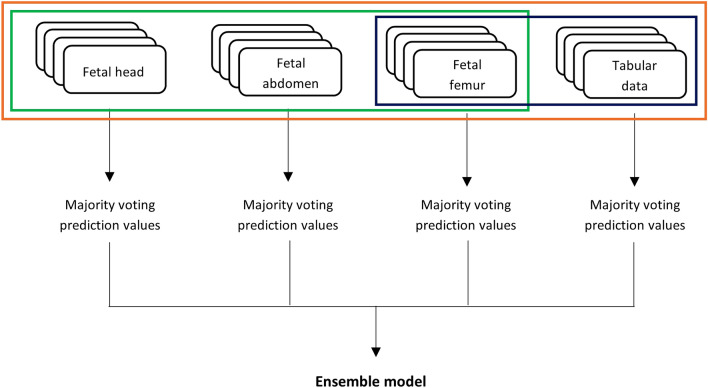
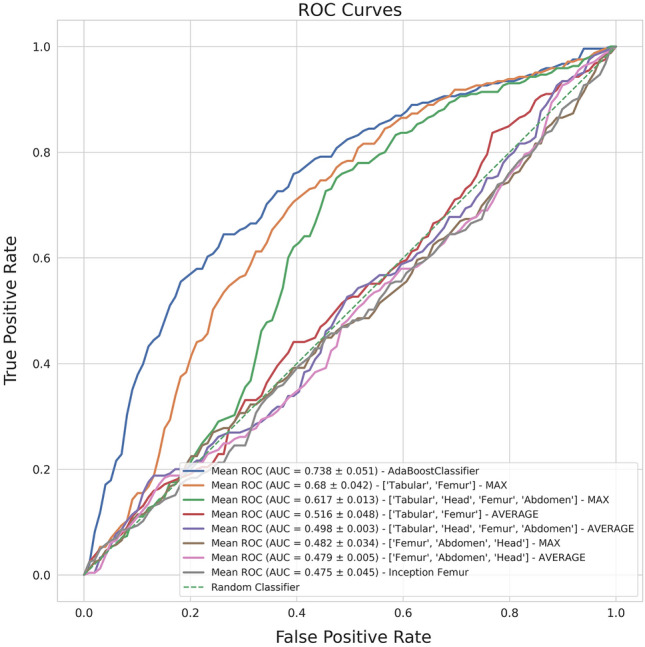
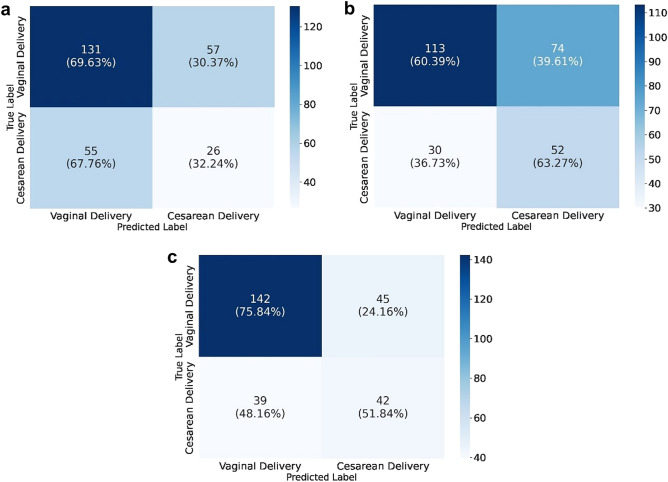
Providing adequate counseling on mode of delivery after induction of labor (IOL) is of utmost importance. Various AI algorithms have been developed for this purpose, but rely on maternal-fetal data, not including ultrasound (US) imaging. We used retrospectively collected clinical data from 808 subjects submitted to IOL, totaling 2024 US images, to train AI models to predict vaginal delivery (VD) and cesarean section (CS) outcomes after IOL. The best overall model used only clinical data (F1-score: 0.736; positive predictive value (PPV): 0.734). The imaging models employed fetal head, abdomen and femur US images, showing limited discriminative results. The best model used femur images (F1-score: 0.594; PPV: 0.580). Consequently, we constructed ensemble models to test whether US imaging could enhance the clinical data model. The best ensemble model included clinical data and US femur images (F1-score: 0.689; PPV: 0.693), presenting a false positive and false negative interesting trade-off. The model accurately predicted CS on 4 additional cases, despite misclassifying 20 additional VD, resulting in a 6.0% decrease in average accuracy compared to the clinical data model. Hence, integrating US imaging into the latter model can be a new development in assisting mode of delivery counseling.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Predicting vaginal delivery after labor induction using machine learning: Development of a multivariable prediction model.Acta Obstet Gynecol Scand. 2025 Jan;104(1):164-173. doi: 10.1111/aogs.14953. Epub 2024 Nov 27. Acta Obstet Gynecol Scand. 2025. PMID: 39601322 Free PMC article.
-
Labor progress determined by ultrasound is different in women requiring cesarean delivery from those who experience a vaginal delivery following induction of labor.Am J Obstet Gynecol. 2019 Oct;221(4):335.e1-335.e18. doi: 10.1016/j.ajog.2019.05.040. Epub 2019 May 30. Am J Obstet Gynecol. 2019. PMID: 31153931
-
Comparison of different methods of measuring angle of progression in prediction of labor outcome.Ultrasound Obstet Gynecol. 2020 Mar;55(3):391-400. doi: 10.1002/uog.21913. Ultrasound Obstet Gynecol. 2020. PMID: 31692170
-
Effects of induction of labor prior to post-term in low-risk pregnancies: a systematic review.JBI Database System Rev Implement Rep. 2019 Feb;17(2):170-208. doi: 10.11124/JBISRIR-2017-003587. JBI Database System Rev Implement Rep. 2019. PMID: 30299344 Free PMC article.
-
Delivery for women with a previous cesarean: guidelines for clinical practice from the French College of Gynecologists and Obstetricians (CNGOF).Eur J Obstet Gynecol Reprod Biol. 2013 Sep;170(1):25-32. doi: 10.1016/j.ejogrb.2013.05.015. Epub 2013 Jun 28. Eur J Obstet Gynecol Reprod Biol. 2013. PMID: 23810846 Review.
Cited by
-
Does infant birthweight percentile identify mothers at risk of severe morbidity? A Canadian population-based cohort study.Matern Health Neonatol Perinatol. 2025 Jul 3;11(1):19. doi: 10.1186/s40748-025-00217-8. Matern Health Neonatol Perinatol. 2025. PMID: 40604901 Free PMC article.
-
Artificial intelligence assisted common maternal fetal planes prediction from ultrasound images based on information fusion of customized convolutional neural networks.Front Med (Lausanne). 2024 Oct 29;11:1486995. doi: 10.3389/fmed.2024.1486995. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39534222 Free PMC article.
-
Artificial Intelligence in Predicting the Mode of Delivery: A Systematic Review.Cureus. 2024 Sep 10;16(9):e69115. doi: 10.7759/cureus.69115. eCollection 2024 Sep. Cureus. 2024. PMID: 39391427 Free PMC article. Review.
References
-
- Organization, W. H. WHO Team—Sexual and Reproductive Health and Research 8 (2015).
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
