

Biomarkers In Prediction of Acute Mesenteric Ischaemia: a prospective multicentre study (BIPAMI study): a study protocol
- PMID: 38961419
- PMCID: PMC11221143
- DOI: 10.1186/s12893-024-02491-3
Biomarkers In Prediction of Acute Mesenteric Ischaemia: a prospective multicentre study (BIPAMI study): a study protocol
Abstract
Background: Acute mesenteric ischaemia (AMI) is a life-threatening disease where early diagnosis is critical to avoid morbidity and mortality from extensive irreversible bowel necrosis. Appropriate prediction of presence of bowel necrosis is currently not available but would help to choose the optimal method of treatment. The study aims to identify combinations of biomarkers that can reliably identify AMI and distinguish between potentially reversible and irreversible bowel ischaemia.
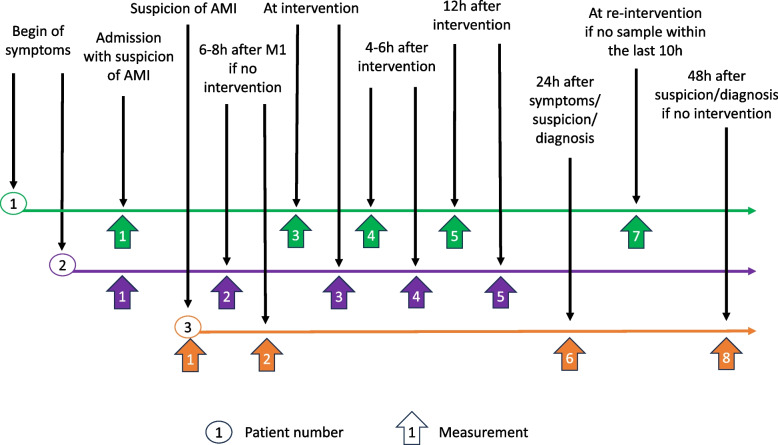
Methods: This is a prospective multicentre study. Adult patients with clinical suspicion of AMI (n = 250) will be included. Blood will be sampled on admission, at and after interventions, or during the first 48 h of suspicion of AMI if no intervention undertaken. Samples will be collected and the following serum or plasma biomarkers measured at Tartu University Hospital laboratory: intestinal fatty acid-binding protein (I-FABP), alpha-glutathione S-transferase (Alpha- GST), interleukin 6 (IL-6), procalcitonin (PCT), ischaemia-modified albumin (IMA), D-lactate, D-dimer, signal peptide-CUB-EGF domain-containing protein 1 (SCUBE-1) and lipopolysaccharide-binding protein (LBP). Additionally, more common laboratory markers will be measured in routine clinical practice at study sites. Diagnosis of AMI will be confirmed by computed tomography angiography, surgery, endoscopy or autopsy. Student's t or Wilcoxon rank tests will be used for comparisons between transmural vs. suspected (but not confirmed) AMI (comparison A), confirmed AMI of any stage vs suspected AMI (comparison B) and non-transmural AMI vs transmural AMI (comparison C). Optimal cut-off values for each comparison will be identified based on the AUROC analysis and likelihood ratios calculated. Positive likelihood ratio > 10 (> 5) and negative likelihood ratio < 0.1 (< 0.2) indicate high (moderate) diagnostic accuracy, respectively. All biomarkers with at least moderate accuracy will be entered as binary covariates (using the best cutoffs) into the multivariable stepwise regression analysis to identify the best combination of biomarkers for all comparisons separately. The best models for each comparison will be used to construct a practical score to distinguish between no AMI, non-transmural AMI and transmural AMI.
Discussion: As a result of this study, we aim to propose a score including set of biomarkers that can be used for diagnosis and decision-making in patients with suspected AMI.
Trial registration: NCT06212921 (Registration Date 19-01-2024).
Keywords: Acute mesenteric ischaemia; Biomarkers; Diagnosis.
© 2024. The Author(s).
Conflict of interest statement
ARB has received speaker or consultancy fees from Nestlé, VIPUN Medical, Nutricia and Fresenius Kabi, and is holding a grant from Estonian Research Council (PRG1255). AF has received speaker fees from B Braun and Fresenius Kabi. AN has received speaker or consultancy fees from Abbvie and Janssen, research funding from MSD-Avenir, and PhD grants from Fondation de l’Avenir and SNFGE. KT, SA, AB, MB, DC, DD, KKa, KKi, IL, VM, MMu, MMä, MP, JS and DV declare no conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
