

POStoperative INTELLiVENT-adaptive support VEntilation in cardiac surgery patients (POSITiVE) II-study protocol of a randomized clinical trial
- PMID: 38961468
- PMCID: PMC11223327
- DOI: 10.1186/s13063-024-08296-2
POStoperative INTELLiVENT-adaptive support VEntilation in cardiac surgery patients (POSITiVE) II-study protocol of a randomized clinical trial
Abstract
Background: One single-center randomized clinical trial showed that INTELLiVENT-adaptive support ventilation (ASV) is superior to conventional ventilation with respect to the quality of ventilation in post-cardiac surgery patients. Other studies showed that this automated ventilation mode reduces the number of manual interventions at the ventilator in various types of critically ill patients. In this multicenter study in patients post-cardiac surgery, we test the hypothesis that INTELLiVENT-ASV is superior to conventional ventilation with respect to the quality of ventilation.
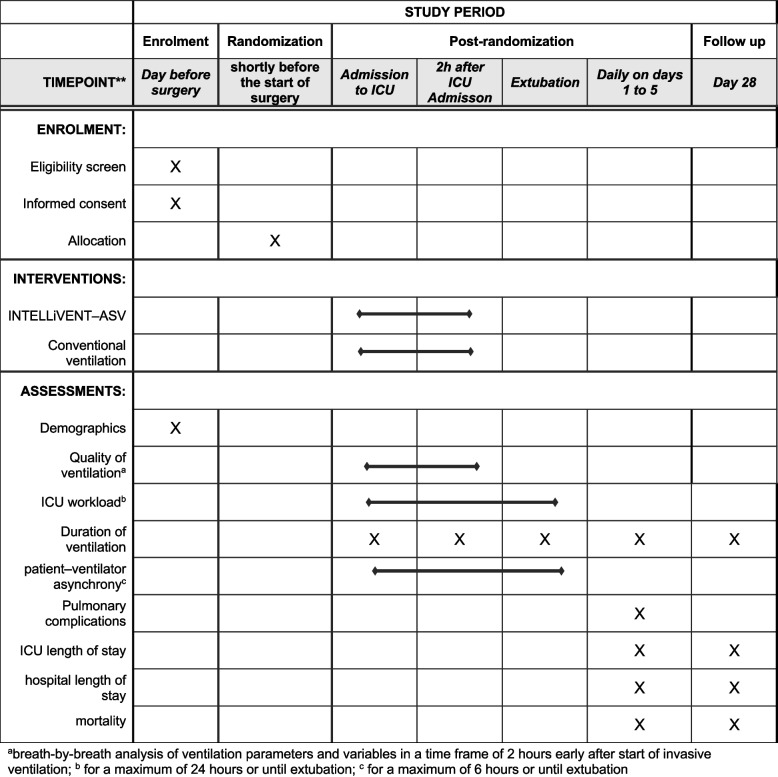
Methods: "POStoperative INTELLiVENT-adaptive support VEntilation in cardiac surgery patients II (POSITiVE II)" is an international, multicenter, two-group randomized clinical superiority trial. In total, 328 cardiac surgery patients will be randomized. Investigators screen patients aged > 18 years of age, scheduled for elective cardiac surgery, and expected to receive postoperative ventilation in the ICU for longer than 2 h. Patients either receive automated ventilation by means of INTELLiVENT-ASV or ventilation that is not automated by means of a conventional ventilation mode. The primary endpoint is quality of ventilation, defined as the proportion of postoperative ventilation time characterized by exposure to predefined optimal, acceptable, and critical (injurious) ventilatory parameters in the first two postoperative hours. One major secondary endpoint is ICU team staff workload, captured by the ventilator software collecting manual settings on alarms. Patient-centered endpoints include duration of postoperative ventilation and length of stay in ICU.
Discussion: POSITiVE II is the first international, multicenter, randomized clinical trial designed to confirm that POStoperative INTELLiVENT-ASV is superior to non-automated conventional ventilation and secondary to determine if this closed-loop ventilation mode reduces ICU team staff workload. The results of POSITiVE II will support intensive care teams in their choices regarding the use of automated ventilation in postoperative care of uncomplicated cardiac surgery patients.
Trial registration: Clinicaltrials.gov NCT06178510 . Registered on December 4, 2023.
Keywords: Automation; Cardiac surgery; Closed-loop; I-ASV; INTELLiVENT-ASV; Intensive care; Invasive ventilation; Mechanical ventilation; Postoperative ventilation; Randomized clinical trial.
© 2024. The Author(s).
Conflict of interest statement
Laura Buiteman–Kruizinga received fees from Hamilton Medical AG for lecturing. Prof Reto Schuepbach declares ongoing studies with Hamilton medical and an education sponsorship. Prof Marcus J. Schultz was Team Leader Medical Research at Hamilton Medical AG, Bonaduz, Switzerland, from January 2022 till January 2023, and receives grants from Zorgonderzoek Medische wetenschappen (ZonMw) in the Netherlands. The other authors declare that they have no competing interests.
Figures
Similar articles
-
Effect of Automated Closed-loop ventilation versus convenTional VEntilation on duration and quality of ventilation in critically ill patients (ACTiVE) - study protocol of a randomized clinical trial.Trials. 2022 Apr 23;23(1):348. doi: 10.1186/s13063-022-06286-w. Trials. 2022. PMID: 35461264 Free PMC article.
-
Comparative analysis of fully automated vs. conventional ventilation in postoperative cardiac surgery patients: Impact on alarms, interventions, and nurse acceptance.Intensive Crit Care Nurs. 2025 Aug;89:103963. doi: 10.1016/j.iccn.2025.103963. Epub 2025 Feb 11. Intensive Crit Care Nurs. 2025. PMID: 39938276 Clinical Trial.
-
Closed-loop ventilation mode (IntelliVent®-ASV) in intensive care unit: a randomized trial.Minerva Anestesiol. 2016 Jun;82(6):657-68. Epub 2016 Mar 8. Minerva Anestesiol. 2016. PMID: 26957117 Clinical Trial.
-
Effectiveness, safety and efficacy of INTELLiVENT-adaptive support ventilation, a closed-loop ventilation mode for use in ICU patients - a systematic review.Expert Rev Respir Med. 2021 Nov;15(11):1403-1413. doi: 10.1080/17476348.2021.1933450. Epub 2021 Jul 31. Expert Rev Respir Med. 2021. PMID: 34047244
-
Effectiveness of Adaptive Support Ventilation in Facilitating Weaning from Mechanical Ventilation in Postoperative Patients.J Cardiothorac Vasc Anesth. 2024 Sep;38(9):1978-1986. doi: 10.1053/j.jvca.2024.04.030. Epub 2024 Apr 24. J Cardiothorac Vasc Anesth. 2024. PMID: 38937174
References
-
- Serpa Neto A, Deliberato RO, Johnson AEW, Bos LD, Amorim P, Pereira SM, et al. Mechanical power of ventilation is associated with mortality in critically ill patients: an analysis of patients in two observational cohorts. Intensive Care Med. 2018;44(11):1914–1922. doi: 10.1007/s00134-018-5375-6. - DOI - PubMed
-
- Urner M, Jüni P, Hansen B, Wettstein MS, Ferguson ND, Fan E. Time-varying intensity of mechanical ventilation and mortality in patients with acute respiratory failure: a registry-based, prospective cohort study. Lancet Respir Med. 2020;8(9):905–913. doi: 10.1016/S2213-2600(20)30325-8. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
