

The impact of norepinephrine dose reporting heterogeneity on mortality prediction in septic shock patients
- PMID: 38961499
- PMCID: PMC11220947
- DOI: 10.1186/s13054-024-05011-0
The impact of norepinephrine dose reporting heterogeneity on mortality prediction in septic shock patients
Abstract
Background: Norepinephrine (NE) is a cornerstone drug in the management of septic shock, with its dose being used clinically as a marker of disease severity and as mortality predictor. However, variations in NE dose reporting either as salt formulations or base molecule may lead to misinterpretation of mortality risks and hinder the process of care.
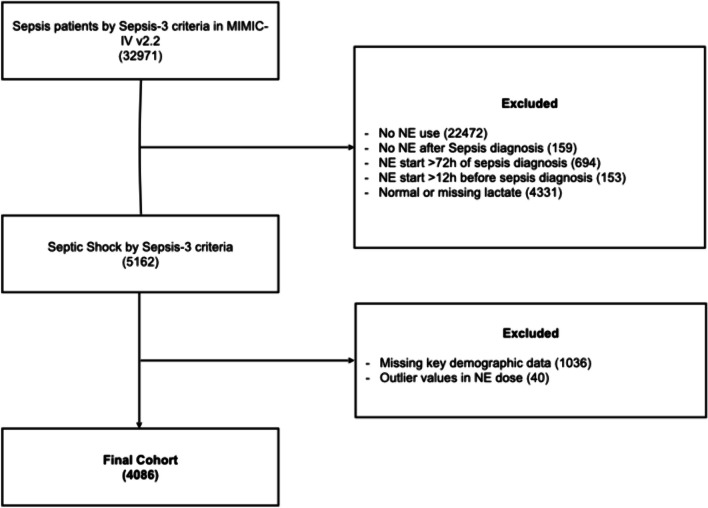
Methods: We conducted a retrospective analysis of the MIMIC-IV database to assess the impact of NE dose reporting heterogeneity on mortality prediction in a cohort of septic shock patients. NE doses were converted from the base molecule to equivalent salt doses, and their ability to predict 28-day mortality at common severity dose cut-offs was compared.
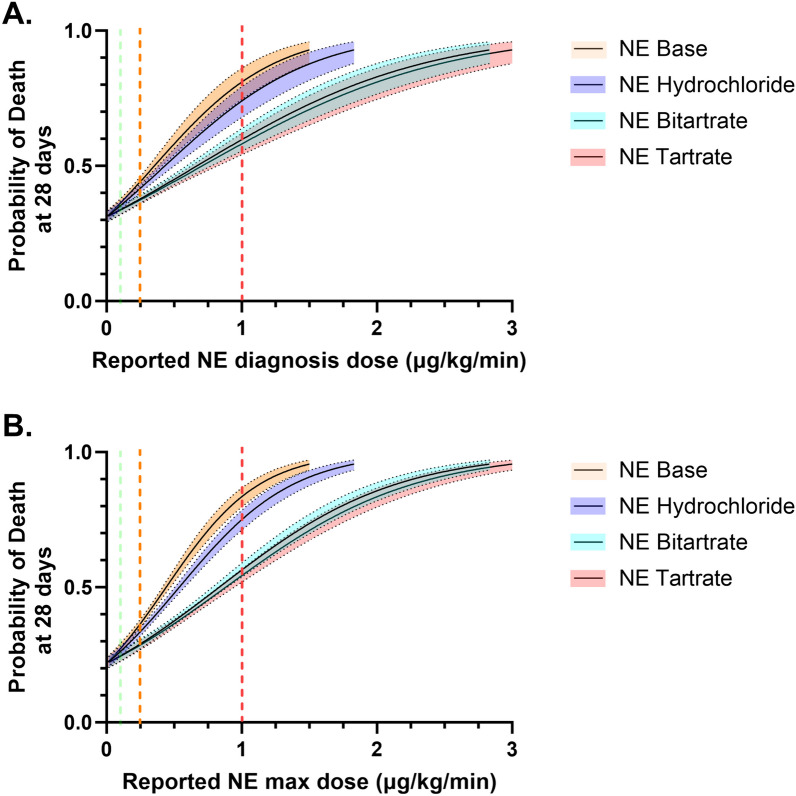
Results: 4086 eligible patients with septic shock were identified, with a median age of 68 [57-78] years, an admission SOFA score of 7 [6-10], and lactate at diagnosis of 3.2 [2.4-5.1] mmol/L. Median peak NE dose at day 1 was 0.24 [0.12-0.42] μg/kg/min, with a 28-day mortality of 39.3%. The NE dose showed significant heterogeneity in mortality prediction depending on which formulation was reported, with doses reported as bitartrate and tartrate presenting 65 (95% CI 79-43)% and 67 (95% CI 80-47)% lower ORs than base molecule, respectively. This divergence in prediction widened at increasing NE doses. When using a 1 μg/kg/min threshold, predicted mortality was 54 (95% CI 52-56)% and 83 (95% CI 80-87)% for tartrate formulation and base molecule, respectively.
Conclusions: Heterogeneous reporting of NE doses significantly affects mortality prediction in septic shock. Standardizing NE dose reporting as base molecule could enhance risk stratification and improve processes of care. These findings underscore the importance of consistent NE dose reporting practices in critical care settings.
Keywords: Mortality prediction; Norepinephrine; Norepinephrine formulation; Septic shock.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
