

Harnessing health information technology to promote equitable care for patients with limited English proficiency and complex care needs
- PMID: 38961501
- PMCID: PMC11223355
- DOI: 10.1186/s13063-024-08254-y
Harnessing health information technology to promote equitable care for patients with limited English proficiency and complex care needs
Abstract
Background: Patients with language barriers encounter healthcare disparities, which may be alleviated by leveraging interpreter skills to reduce cultural, language, and literacy barriers through improved bidirectional communication. Evidence supports the use of in-person interpreters, especially for interactions involving patients with complex care needs. Unfortunately, due to interpreter shortages and clinician underuse of interpreters, patients with language barriers frequently do not get the language services they need or are entitled to. Health information technologies (HIT), including artificial intelligence (AI), have the potential to streamline processes, prompt clinicians to utilize in-person interpreters, and support prioritization.
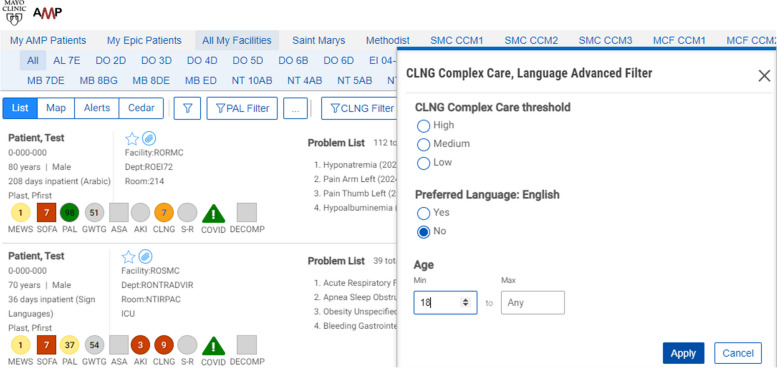
Methods: From May 1, 2023, to June 21, 2024, a single-center stepped wedge cluster randomized trial will be conducted within 35 units of Saint Marys Hospital & Methodist Hospital at Mayo Clinic in Rochester, Minnesota. The units include medical, surgical, trauma, and mixed ICUs and hospital floors that admit acute medical and surgical care patients as well as the emergency department (ED). The transitions between study phases will be initiated at 60-day intervals resulting in a 12-month study period. Units in the control group will receive standard care and rely on clinician initiative to request interpreter services. In the intervention group, the study team will generate a daily list of adult inpatients with language barriers, order the list based on their complexity scores (from highest to lowest), and share it with interpreter services, who will send a secure chat message to the bedside nurse. This engagement will be triggered by a predictive machine-learning algorithm based on a palliative care score, supplemented by other predictors of complexity including length of stay and level of care as well as procedures, events, and clinical notes.
Discussion: This pragmatic clinical trial approach will integrate a predictive machine-learning algorithm into a workflow process and evaluate the effectiveness of the intervention. We will compare the use of in-person interpreters and time to first interpreter use between the control and intervention groups.
Trial registration: NCT05860777. May 16, 2023.
Keywords: AI; Complex care needs; Complexity score; Healthcare disparities; In-person interpreter; Language services; Non-English language preference (NELP).
© 2024. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
The authors declare no competing interests.
Figures
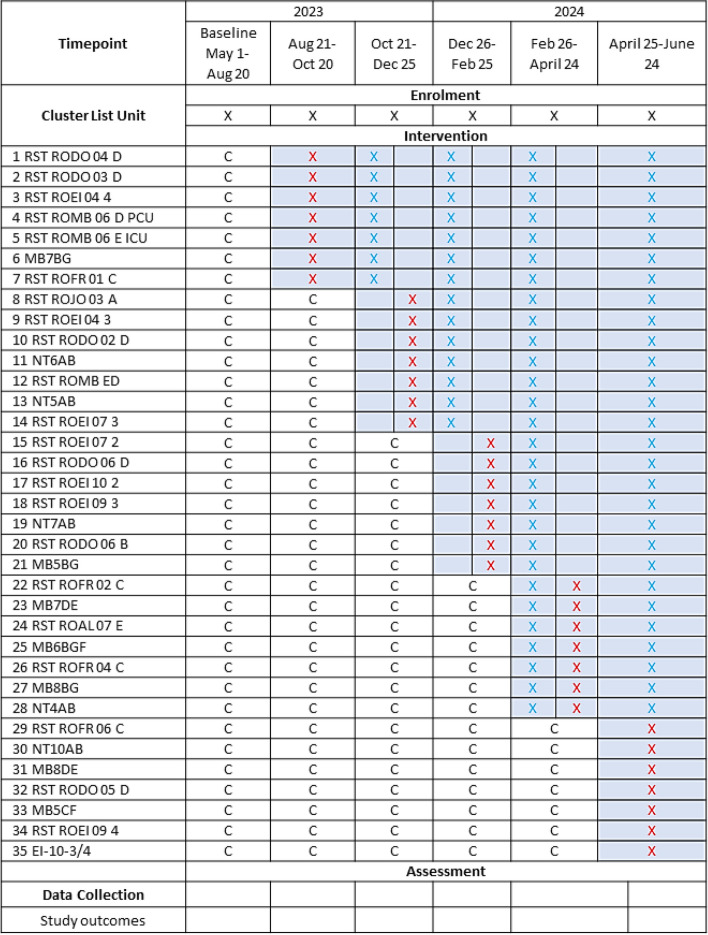
 in 60-day steps. Usual care is denoted by “c”
in 60-day steps. Usual care is denoted by “c”Similar articles
-
Using artificial intelligence to promote equitable care for inpatients with language barriers and complex medical needs: clinical stakeholder perspectives.J Am Med Inform Assoc. 2024 Feb 16;31(3):611-621. doi: 10.1093/jamia/ocad224. J Am Med Inform Assoc. 2024. PMID: 38099504 Free PMC article.
-
Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review.JBI Evid Synth. 2020 Jul;18(7):1360-1388. doi: 10.11124/JBISRIR-D-19-00300. JBI Evid Synth. 2020. PMID: 32813387
-
Patient Time Spent With Professional Medical Interpreters and the Care Experiences of Patients With Limited English Proficiency.J Prim Care Community Health. 2024 Jan-Dec;15:21501319241264168. doi: 10.1177/21501319241264168. J Prim Care Community Health. 2024. PMID: 38912573 Free PMC article.
-
The use of interpreter services and its barriers faced by hospital staff when accessing interpreters for patients with low English proficiency during the COVID-19 pandemic.Health Promot J Austr. 2024 Oct;35(4):1184-1193. doi: 10.1002/hpja.850. Epub 2024 Feb 25. Health Promot J Austr. 2024. PMID: 38402882
-
Language interpreter utilization in the emergency department setting: a clinical review.J Health Care Poor Underserved. 2008 May;19(2):352-62. doi: 10.1353/hpu.0.0019. J Health Care Poor Underserved. 2008. PMID: 18469408 Review.
Cited by
-
The Use of Artificial Intelligence in Palliative Care Communication: A Narrative Review.Cureus. 2025 Mar 13;17(3):e80524. doi: 10.7759/cureus.80524. eCollection 2025 Mar. Cureus. 2025. PMID: 40225512 Free PMC article. Review.
References
-
- LEP.gov.https://www.lep.gov/sites/lep/files/media/document/2020-03/042511_QA_LEP.... Accessed 11/12/2020.
-
- American Community Survey, Detailed languages spoken at home and ability to speak English for the population 5 years and over. 2009-2013; https://www.census.gov/data.html. Accessed 5/1/2019.
-
- Regenstein M, et al. et al. Hospital language services: quality improvement and performance measures. In: Henriksen K, et al.et al., editors. Advances in patient safety: new directions and alternative approaches (Vol. 2: Culture and Redesign) Rockville (MD): Agency for Healthcare Research and Quality (US); 2008. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
