

Optimizing intrauterine insemination: A systematic review and meta-analysis of the effectiveness and safety of clinical treatment add-ons
- PMID: 38961556
- PMCID: PMC11426219
- DOI: 10.1111/aogs.14858
Optimizing intrauterine insemination: A systematic review and meta-analysis of the effectiveness and safety of clinical treatment add-ons
Abstract
Introduction: Intrauterine insemination (IUI) is one of the most widespread fertility treatments. However, IUI protocols vary significantly amongst fertility clinics. Various add-on interventions have been proposed to boost success rates. These are mostly chosen arbitrarily or empirically. The aim of this systematic review and meta-analysis is to assess the effectiveness and safety of add-on interventions to the standard IUI protocol and to provide evidence-based recommendations on techniques used to optimize the clinical outcomes of IUI treatment.
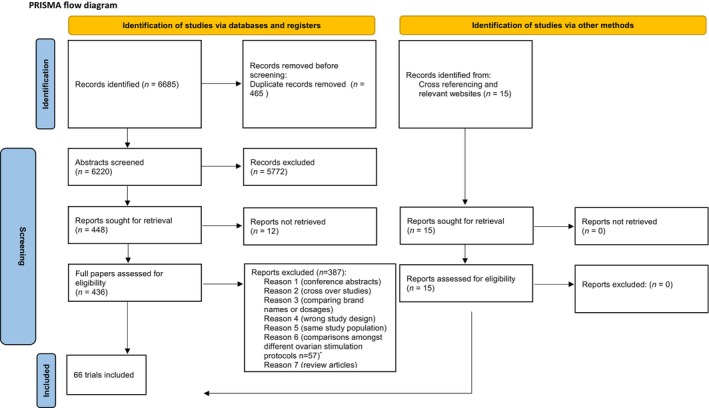
Material and methods: Systematic review and meta-analyses were performed in accordance with PRISMA guidelines. A computerized literature search was performed from database inception to May 2023. Randomized controlled trials (RCTs) were included reporting on couples/single women undergoing IUI with any protocol for any indication using partner's or donor sperm. A meta-analysis based on random effects was performed for each outcome and add-on. Three authors independently assessed the trials for quality and risk of bias and overall certainty of evidence. Uncertainties were resolved through consensus. Primary outcomes were ongoing pregnancy rate (OPR) or live birth rate (LBR) per cycle/per woman randomized. Registration number PROSPERO: CRD42022300857.
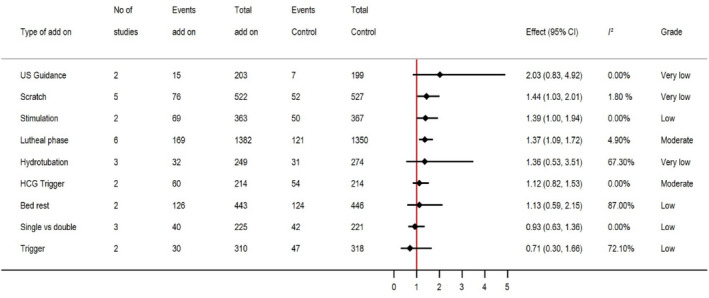
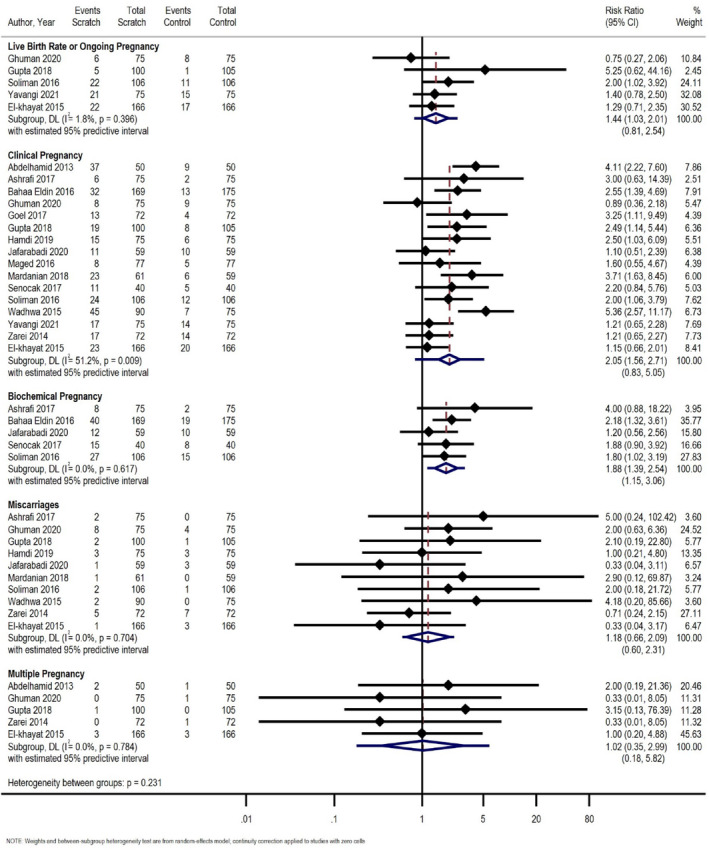
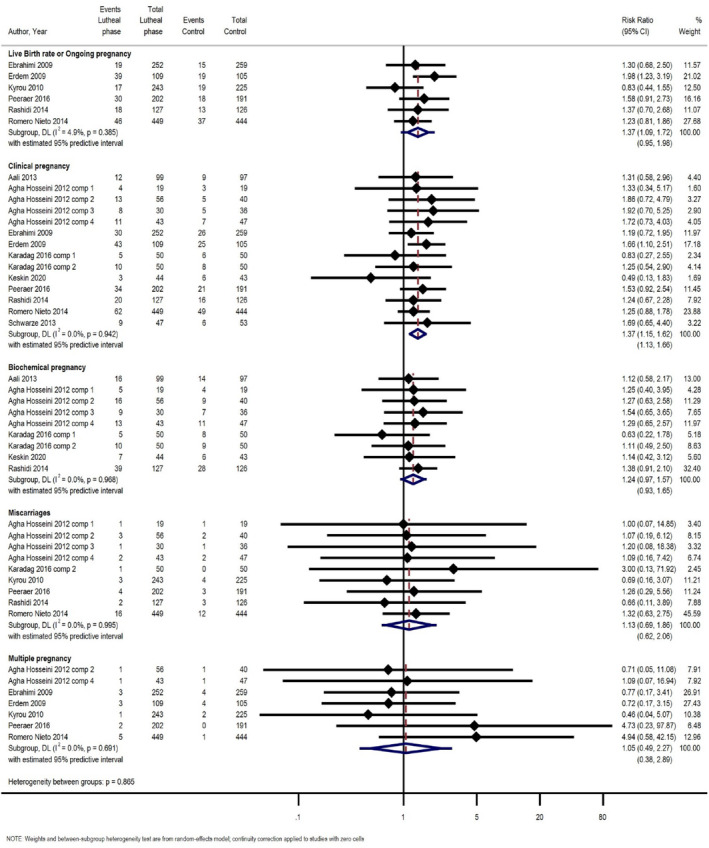
Results: Sixty-six RCTs were included in the analysis (16 305 participants across 20 countries). Vaginal progesterone as luteal phase support in stimulated cycles was found to significantly increase LBR/OPR (RR 1.37, 95% CI 1.09-1.72, I2 = 4.9%) (moderate/low certainty of the evidence). Endometrial scratch prior/during stimulated IUI cycles may increase LBR/OPR (RR 1.44, 95% CI 1.03-2.01, I2 = 1.8%), but evidence is very uncertain. Results from two studies suggest that follicular phase ovarian stimulation increases LBR/OPR (RR 1.39, 95% CI 1.00-1.94, I2 = 0%) (low certainty of evidence). No significant difference was seen for the primary outcome for the other studied interventions.
Conclusions: The findings of this systematic review and meta-analysis suggest that vaginal luteal phase progesterone support probably improves LBR/OPR in stimulated IUI treatments. In view of moderate/low certainty of the evidence more research is needed for solid conclusions. Further research is also recommended for the use of endometrial scratch and ovarian stimulation. Future studies should report on results according to subfertility background as it is possible that different add-ons could benefit specific patient groups.
Keywords: IUI; add‐ons; bed rest; insemination; progesterone; scratch.
© 2024 The Authors. Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
The authors have no competing interests to declare that are relevant to the content of this article.
Figures
Similar articles
-
Luteal phase support for women trying to conceive by intrauterine insemination or sexual intercourse.Cochrane Database Syst Rev. 2022 Aug 24;8(8):CD012396. doi: 10.1002/14651858.CD012396.pub2. Cochrane Database Syst Rev. 2022. PMID: 36000704 Free PMC article.
-
Endometrial injury for pregnancy following sexual intercourse or intrauterine insemination.Cochrane Database Syst Rev. 2022 Oct 24;10(10):CD011424. doi: 10.1002/14651858.CD011424.pub4. Cochrane Database Syst Rev. 2022. PMID: 36278845 Free PMC article.
-
Endometrial injury for pregnancy following sexual intercourse or intrauterine insemination.Cochrane Database Syst Rev. 2016 Jun 14;(6):CD011424. doi: 10.1002/14651858.CD011424.pub2. Cochrane Database Syst Rev. 2016. Update in: Cochrane Database Syst Rev. 2021 Mar 18;3:CD011424. doi: 10.1002/14651858.CD011424.pub3. PMID: 27296541 Updated.
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Assisted reproductive technologies for male subfertility.Cochrane Database Syst Rev. 2016 Feb 26;2(2):CD000360. doi: 10.1002/14651858.CD000360.pub5. Cochrane Database Syst Rev. 2016. PMID: 26915339 Free PMC article.
References
-
- Cohen MR. Intrauterine insemination. Int J Fertil. 1962;7:235‐240. - PubMed
-
- Calhaz‐Jorge C, de Geyter C, Kupka MS, et al. Assisted reproductive technology in Europe, 2013: results generated from European registers by ESHRE. Hum Reprod. 2017;32:1957‐1973. - PubMed
-
- Osuna C, Matorras R, Rodriguez‐Escudero FJ, Pijoan JI. The heterogeneity of randomized, controlled trials of intrauterine insemination. Fertil Steril. 2004;82:34‐35. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
