

Validation of Artificial Intelligence in the Classification of Adolescent Idiopathic Scoliosis and the Compairment to Clinical Manual Handling
- PMID: 38961674
- PMCID: PMC11293916
- DOI: 10.1111/os.14144
Validation of Artificial Intelligence in the Classification of Adolescent Idiopathic Scoliosis and the Compairment to Clinical Manual Handling
Abstract
Objective: The accurate measurement of Cobb angles is crucial for the effective clinical management of patients with adolescent idiopathic scoliosis (AIS). The Lenke classification system plays a pivotal role in determining the appropriate fusion levels for treatment planning. However, the presence of interobserver variability and time-intensive procedures presents challenges for clinicians. The purpose of this study is to compare the measurement accuracy of our developed artificial intelligence measurement system for Cobb angles and Lenke classification in AIS patients with manual measurements to validate its feasibility.
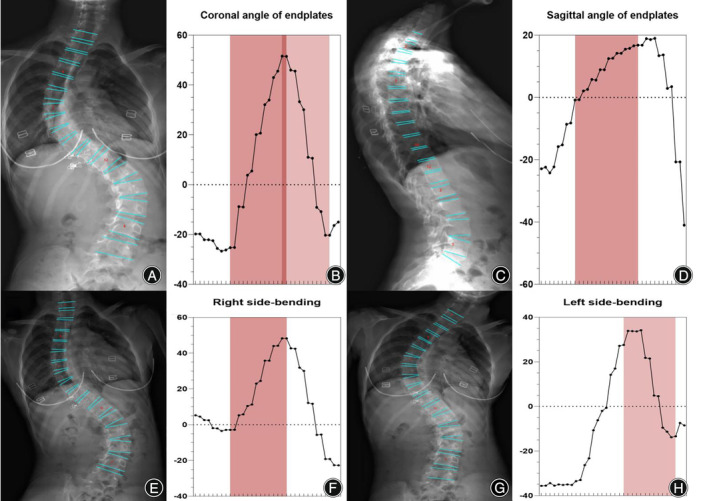
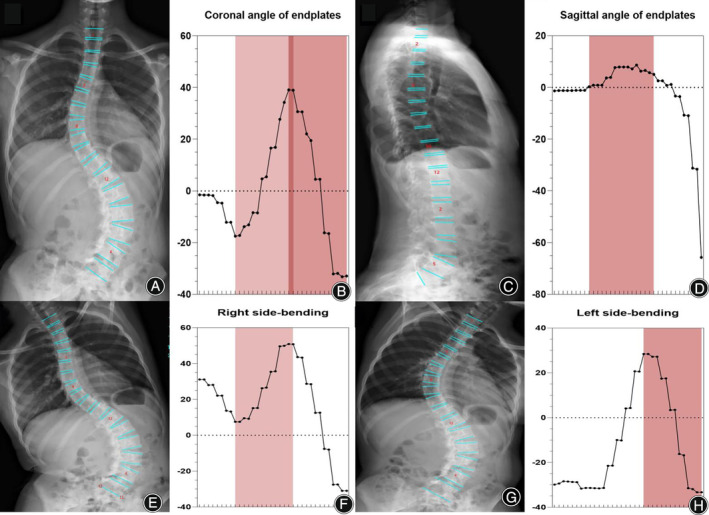
Methods: An artificial intelligence (AI) system measured the Cobb angle of AIS patients using convolutional neural networks, which identified the vertebral boundaries and sequences, recognized the upper and lower end vertebras, and estimated the Cobb angles of the proximal thoracic, main thoracic, and thoracolumbar/lumbar curves sequentially. Accordingly, the Lenke classifications of scoliosis were divided by oscillogram and defined by the AI system. Furthermore, a man-machine comparison (n = 300) was conducted for senior spine surgeons (n = 2), junior spine surgeons (n = 2), and the AI system for the image measurements of proximal thoracic (PT), main thoracic (MT), thoracolumbar/lumbar (TL/L), thoracic sagittal profile T5-T12, bending views PT, bending views MT, bending views TL/L, the Lenke classification system, the lumbar modifier, and sagittal thoracic alignment.
Results: In the AI system, the calculation time for each patient's data was 0.2 s, while the measurement time for each surgeon was 23.6 min. The AI system showed high accuracy in the recognition of the Lenke classification and had high reliability compared to senior doctors (ICC 0.962).
Conclusion: The AI system has high reliability for the Lenke classification and is a potential auxiliary tool for spinal surgeons.
Keywords: Artificial Intelligence; Cobb Angle; Deep Learning; Lenke Classification; Scoliosis; Spine.
© 2024 The Author(s). Orthopaedic Surgery published by Tianjin Hospital and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors declare no competing financial or non‐financial interests. No potential conflict of interest was reported by the authors.
Figures







Similar articles
-
The effectiveness of selective thoracic fusion for treating adolescent idiopathic scoliosis: a systematic review protocol.JBI Database System Rev Implement Rep. 2015 Nov;13(11):4-16. doi: 10.11124/jbisrir-2015-2338. JBI Database System Rev Implement Rep. 2015. PMID: 26657460
-
Preoperative supine traction radiographs often result in higher Lenke classifications than supine bending radiographs in adolescent idiopathic scoliosis.Spine Deform. 2021 Jul;9(4):1049-1052. doi: 10.1007/s43390-020-00271-6. Epub 2021 Jan 13. Spine Deform. 2021. PMID: 33442850
-
Selective versus nonselective thoracic fusion in Lenke 1C curves: a meta-analysis of baseline characteristics and postoperative outcomes.J Neurosurg Spine. 2015 Dec;23(6):721-30. doi: 10.3171/2015.1.SPINE141020. Epub 2015 Aug 28. J Neurosurg Spine. 2015. PMID: 26315956
-
Lenke classification system of adolescent idiopathic scoliosis: treatment recommendations.Instr Course Lect. 2005;54:537-42. Instr Course Lect. 2005. PMID: 15948478 Review.
-
Selective Thoracic Fusion of Lenke I and II Curves Affects Sagittal Profiles But Not Sagittal or Spinopelvic Alignment: A Case-Control Study.Spine (Phila Pa 1976). 2015 Jun 15;40(12):926-34. doi: 10.1097/BRS.0000000000000861. Spine (Phila Pa 1976). 2015. PMID: 26067149 Review.
Cited by
-
Radiation-free 3D assessment of back height differences via three-dimensional depth sensing in adolescent idiopathic scoliosis: prospective, single-center, observational study.Eur Spine J. 2025 Jul 21. doi: 10.1007/s00586-025-09154-8. Online ahead of print. Eur Spine J. 2025. PMID: 40689983
-
Management of adolescent scoliosis: a comprehensive review of etiology and rehabilitation.Front Pediatr. 2025 Jul 16;13:1596400. doi: 10.3389/fped.2025.1596400. eCollection 2025. Front Pediatr. 2025. PMID: 40740816 Free PMC article. Review.
-
Deep learning based decision-making and outcome prediction for adolescent idiopathic scoliosis patients with posterior surgery.Sci Rep. 2025 Jan 27;15(1):3389. doi: 10.1038/s41598-025-87370-4. Sci Rep. 2025. PMID: 39870730 Free PMC article.
-
A 20-year research trend analysis of the artificial intelligence on scoliosis using bibliometric methods.Front Pediatr. 2025 Aug 13;13:1531827. doi: 10.3389/fped.2025.1531827. eCollection 2025. Front Pediatr. 2025. PMID: 40881800 Free PMC article. Review.
-
A novel artificial Intelligence-Based model for automated Lenke classification in adolescent idiopathic scoliosis.Eur Spine J. 2025 Jul 11. doi: 10.1007/s00586-025-09106-2. Online ahead of print. Eur Spine J. 2025. PMID: 40643671
References
-
- Cobb JR. Scoliosis; quo vadis. J Bone Jt Surg Am. 1958;40:507–510. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
