

Craniopharyngioma: A comprehensive review of the clinical presentation, radiological findings, management, and future Perspective
- PMID: 38961911
- PMCID: PMC11219339
- DOI: 10.1016/j.heliyon.2024.e32112
Craniopharyngioma: A comprehensive review of the clinical presentation, radiological findings, management, and future Perspective
Abstract
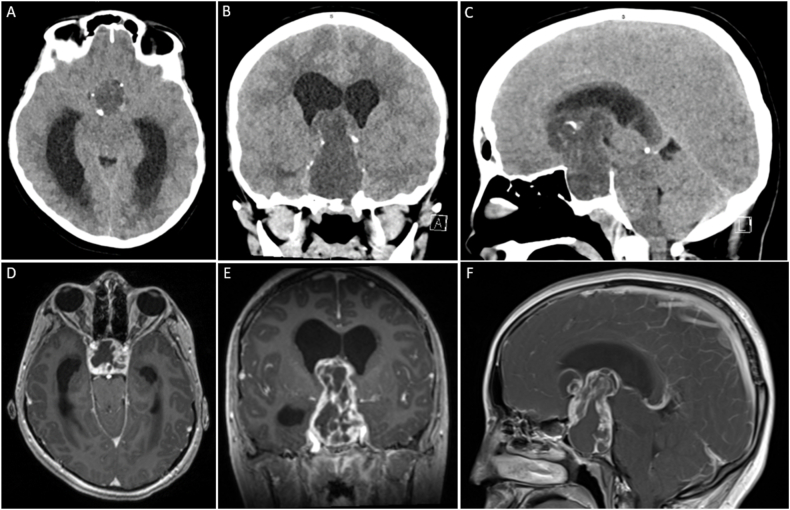
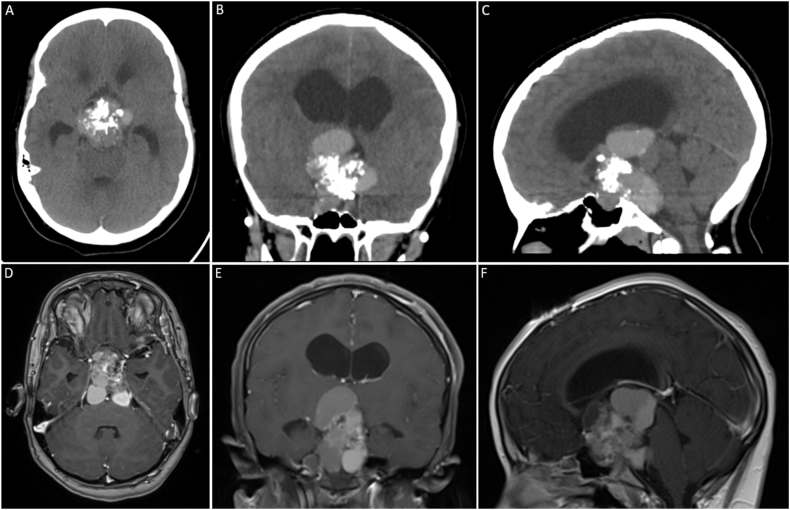
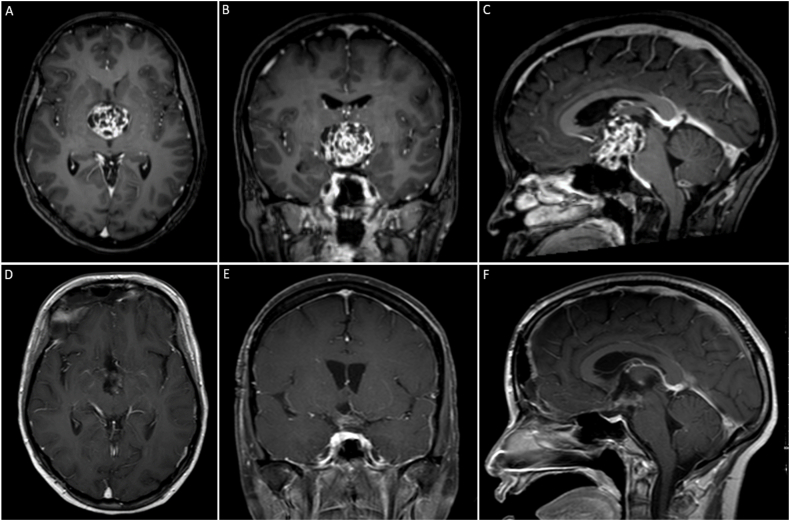
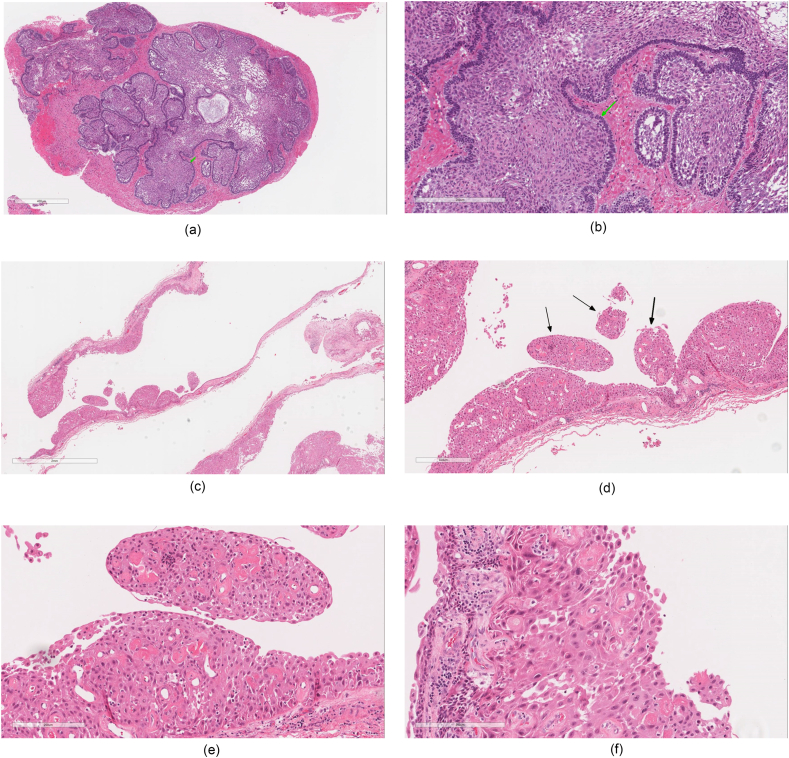
Craniopharyngioma (CP) is a rare intracranial tumor arising from the epithelial remnants of Rathke's pouch, most frequently originating in the sellar/parasellar region. Histologically, CP is a benign low-grade tumor (WHO grade 1) with two distinct phenotypes: adamantinomatous CP (ACP) and papillary CP (PCP). Craniopharyngioma constitutes 1-3% of all primary intracranial tumors in adults and 5-10 % of intracranial tumors in children. The annual incidence ranges from 0.13 to 2 per 100,000 population per year with no gender predilection. Due to its unique anatomical locations, the most frequently reported clinical manifestations are headache, visual impairment, nausea/vomiting, and endocrine deficiencies resulting in sexual dysfunction in adults and growth failure in children. Growth hormone deficiency is the most predominant endocrinological disturbance associated with craniopharyngioma. Computed tomography (CT) is gold standard to detect calcifications in CP tissue (found in 90 % of these tumors). Magnetic Resonance Imaging (MRI) further characterizes craniopharyngiomas and helps to narrow down the differential diagnoses. In almost all craniopharyngioma cases, surgery is indicated to: establish the diagnosis, relieve mass-related symptoms, and remove as much tumor as is safely possible. Recent neurosurgical technical advances, including innovative surgical approaches, detailed radiotherapy protocols, targeted therapy, replacement of lost hormonal functions and quality of life all have the potential to improve the outcome of patients with craniopharyngioma. In this article, we present extensive literature on craniopharyngioma clinical presentation, radiological findings, management, and future prospective. The present article helps to identify further research areas that set the basis for the management of such a complex tumor.
Keywords: Craniopharyngioma; Endocrine; Hormone; Review; Tumor.
© 2024 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Recent advances in craniopharyngioma pathophysiology and emerging therapeutic approaches.Front Endocrinol (Lausanne). 2025 May 13;16:1562942. doi: 10.3389/fendo.2025.1562942. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40433410 Free PMC article. Review.
-
Craniopharyngioma in Pediatrics and Adults.Adv Exp Med Biol. 2023;1405:299-329. doi: 10.1007/978-3-031-23705-8_11. Adv Exp Med Biol. 2023. PMID: 37452943
-
CRANIOPHARYNGIOMA - CLINICAL AND THERAPEUTIC OUTCOME DATA IN A MIXED COHORT OF ADULT AND PAEDIATRIC CASES.Acta Endocrinol (Buchar). 2018 Oct-Dec;14(4):549-555. doi: 10.4183/aeb.2018.549. Acta Endocrinol (Buchar). 2018. PMID: 31149311 Free PMC article.
-
A Histopathological Journey Through Adamantinomatous Craniopharyngioma: A Case Report.Cureus. 2024 Aug 1;16(8):e65917. doi: 10.7759/cureus.65917. eCollection 2024 Aug. Cureus. 2024. PMID: 39221395 Free PMC article.
-
Advances in the Management of Craniopharyngioma: A Narrative Review of Recent Developments and Clinical Strategies.J Clin Med. 2025 Feb 9;14(4):1101. doi: 10.3390/jcm14041101. J Clin Med. 2025. PMID: 40004632 Free PMC article. Review.
Cited by
-
Perioperative Management of a Child With Pre-existing Diabetes Insipidus Undergoing Craniopharyngioma Excision: A Case Report.Cureus. 2024 Nov 12;16(11):e73518. doi: 10.7759/cureus.73518. eCollection 2024 Nov. Cureus. 2024. PMID: 39669816 Free PMC article.
-
Molecular subtypes of adamantinomatous craniopharyngiomas.Neuro Oncol. 2025 Jun 21;27(5):1180-1192. doi: 10.1093/neuonc/noaf030. Neuro Oncol. 2025. PMID: 39898434 Free PMC article. Review.
-
Beyond Epistaxis: A Rare Case of Ectopic Sinonasal Adamantinomatous Craniopharyngioma.Cureus. 2024 Sep 1;16(9):e68357. doi: 10.7759/cureus.68357. eCollection 2024 Sep. Cureus. 2024. PMID: 39355486 Free PMC article.
-
Targeted treatment for craniopharyngioma.J Neurooncol. 2025 May;172(3):503-513. doi: 10.1007/s11060-025-04942-0. Epub 2025 Feb 14. J Neurooncol. 2025. PMID: 39951179 Review.
-
Effectiveness of bariatric surgery on acquired hypothalamic obesity: a systematic review and meta-analysis.Endocr Connect. 2024 Nov 26;13(12):e240493. doi: 10.1530/EC-24-0493. Print 2024 Dec 1. Endocr Connect. 2024. PMID: 39404706 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
