

Dissecting gastric cancer heterogeneity and exploring therapeutic strategies using bulk and single-cell transcriptomic analysis and experimental validation of tumor microenvironment and metabolic interplay
- PMID: 38962317
- PMCID: PMC11220201
- DOI: 10.3389/fphar.2024.1355269
Dissecting gastric cancer heterogeneity and exploring therapeutic strategies using bulk and single-cell transcriptomic analysis and experimental validation of tumor microenvironment and metabolic interplay
Abstract
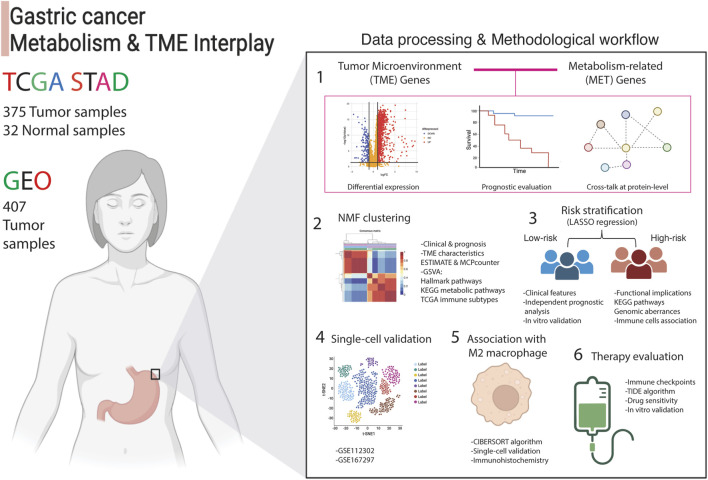
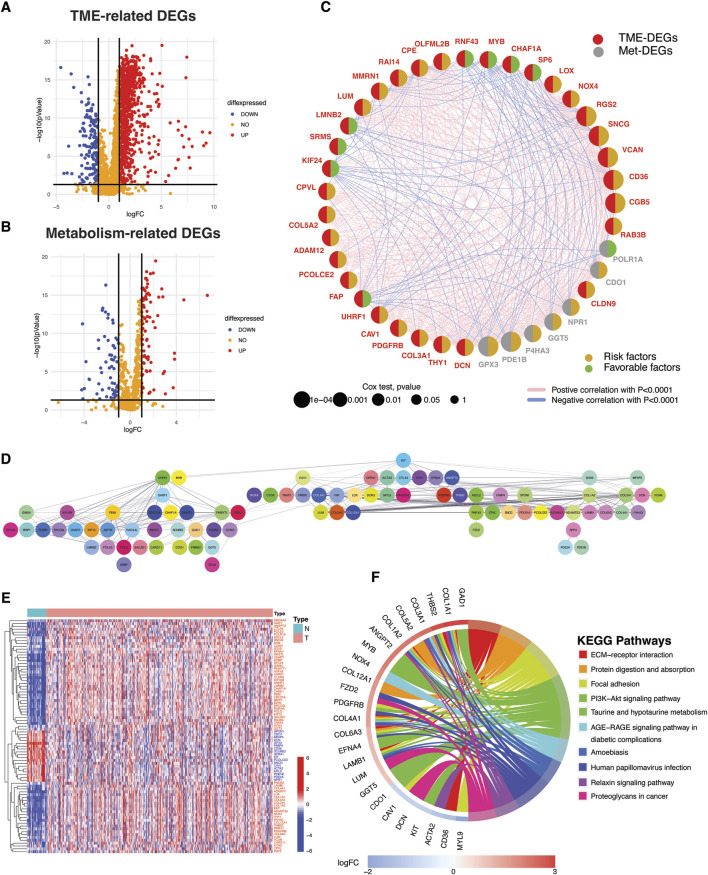
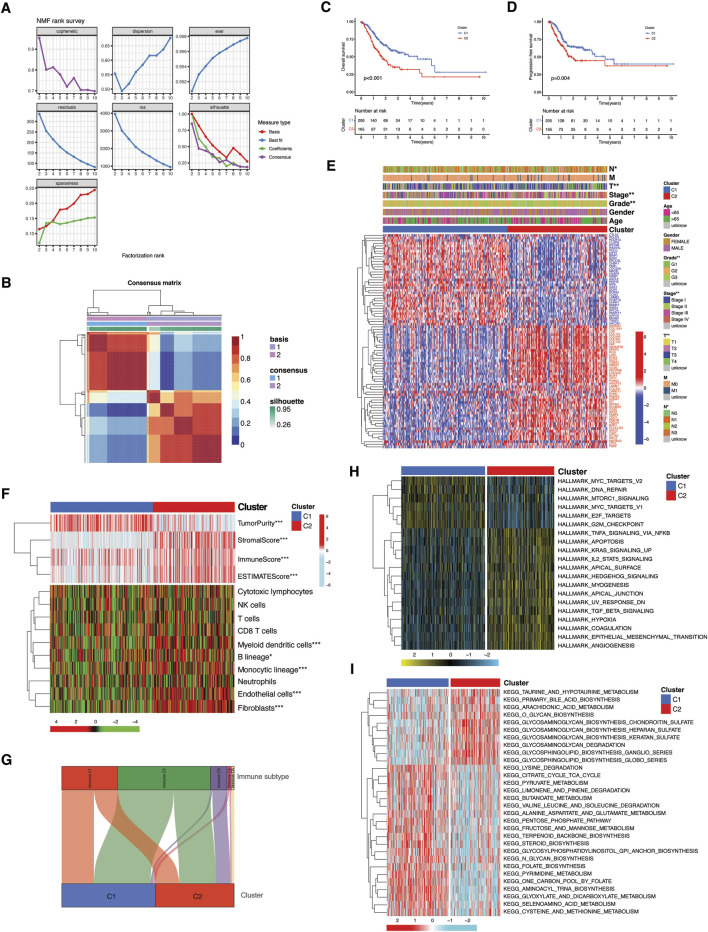
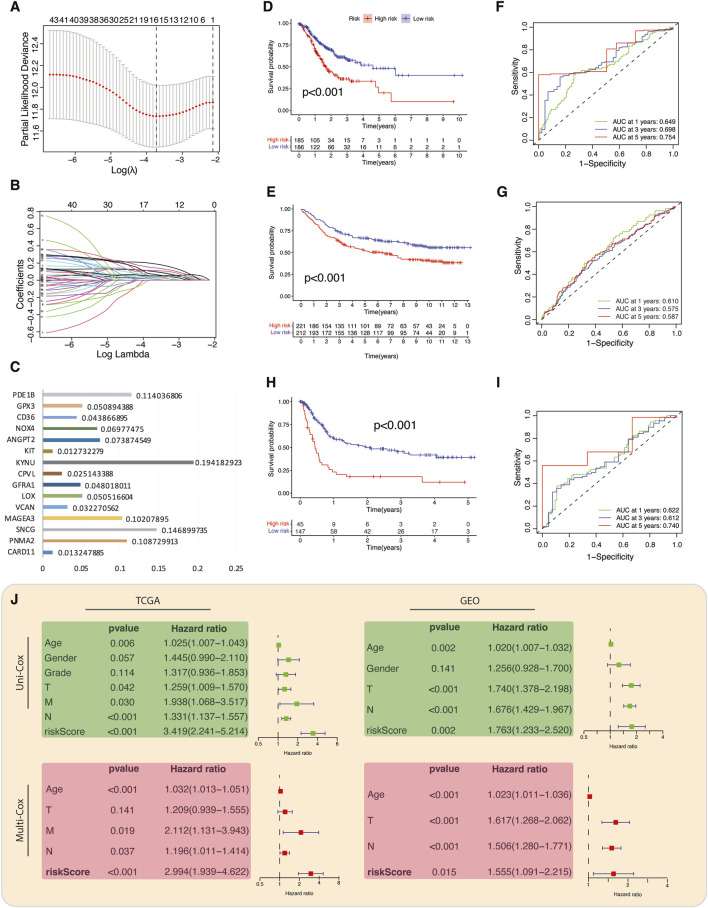
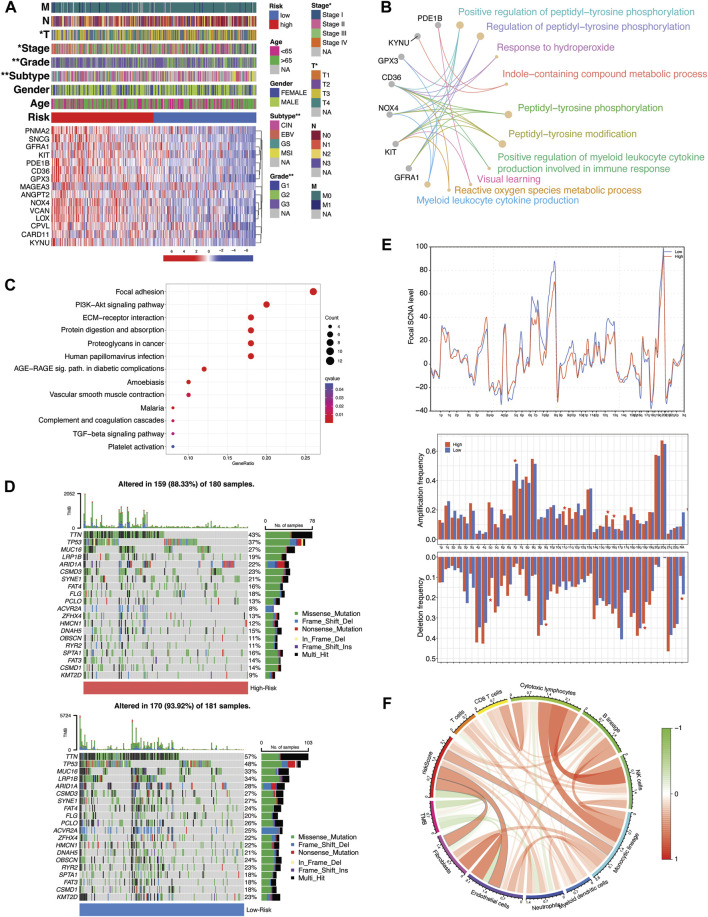
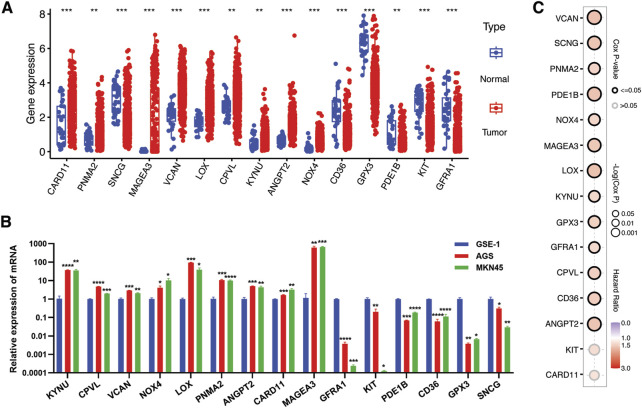
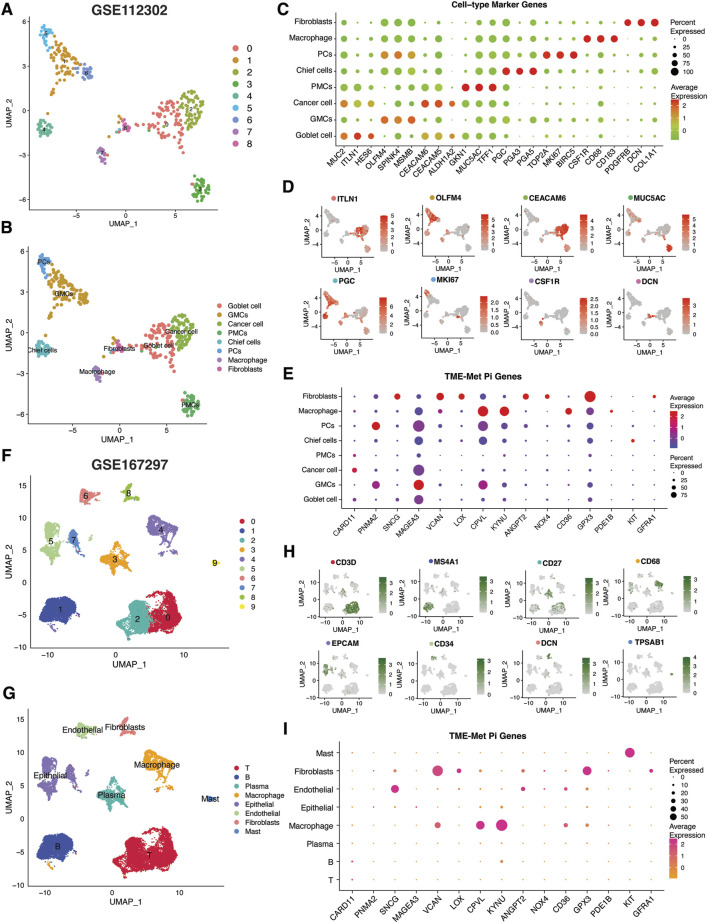
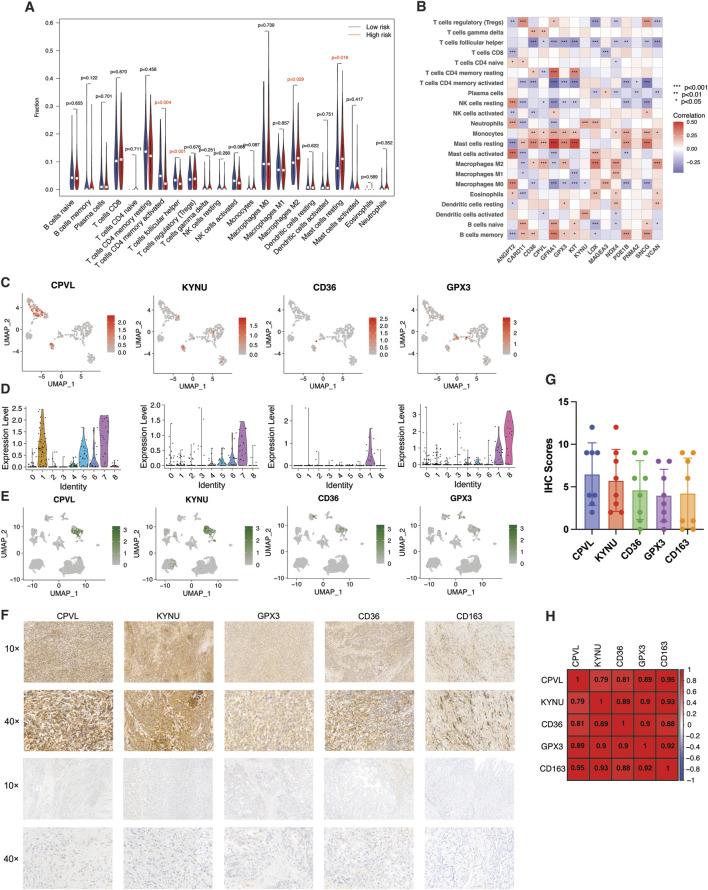
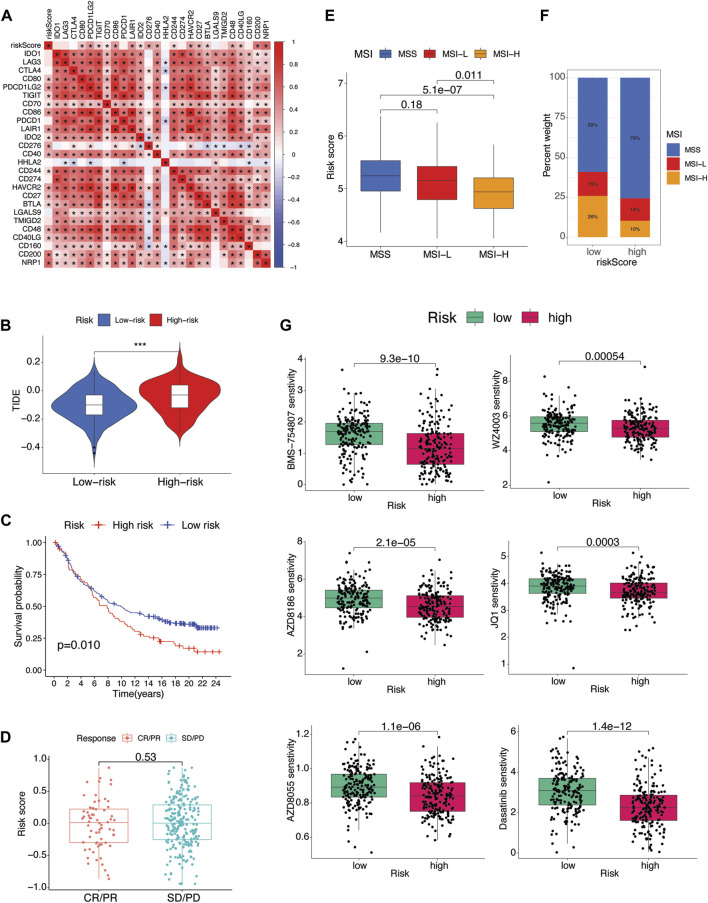
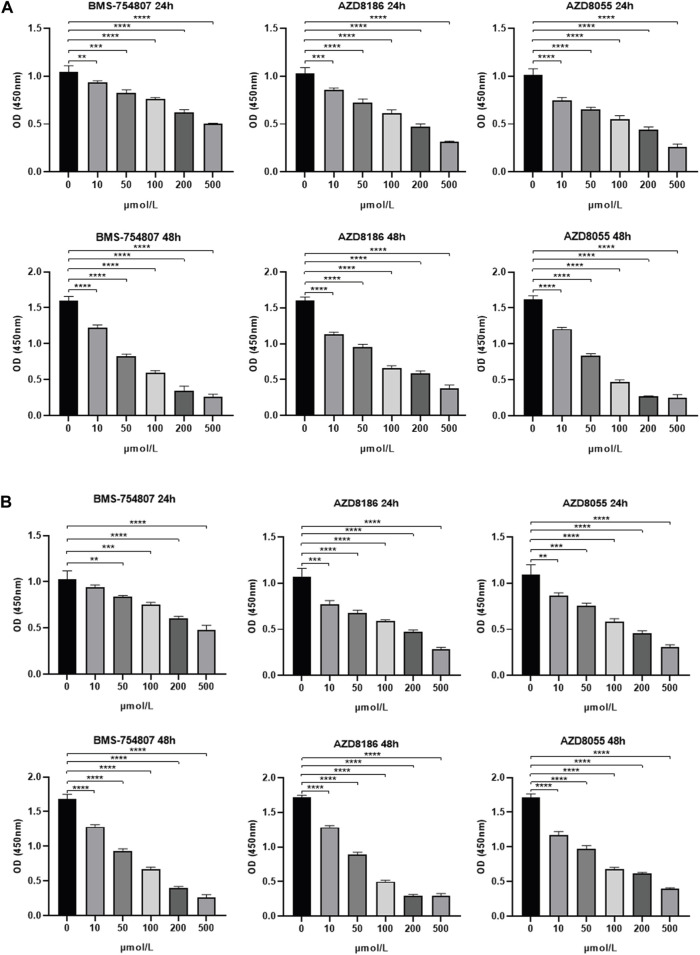
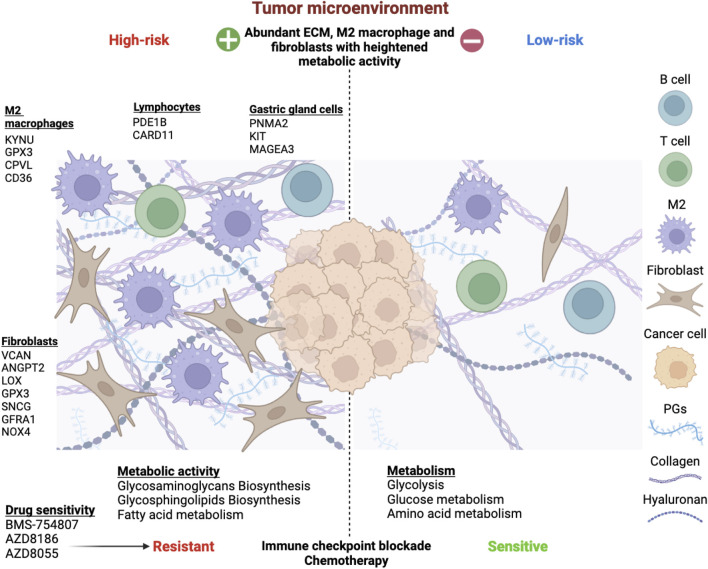
Gastric cancer, the fifth most prevalent cancer worldwide, is often diagnosed in advanced stages with limited treatment options. Examining the tumor microenvironment (TME) and its metabolic reprogramming can provide insights for better diagnosis and treatment. This study investigates the link between TME factors and metabolic activity in gastric cancer using bulk and single-cell RNA-sequencing data. We identified two molecular subtypes in gastric cancer by analyzing the distinct expression patterns of 81 prognostic genes related to the TME and metabolism, which exhibited significant protein-level interactions. The high-risk subtype had increased stromal content, fibroblast and M2 macrophage infiltration, elevated glycosaminoglycans/glycosphingolipids biosynthesis, and fat metabolism, along with advanced clinicopathological features. It also exhibited low mutation rates and microsatellite instability, associating it with the mesenchymal phenotype. In contrast, the low-risk group showed higher tumor content and upregulated protein and sugar metabolism. We identified a 15-gene prognostic signature representing these characteristics, including CPVL, KYNU, CD36, and GPX3, strongly correlated with M2 macrophages, validated through single-cell analysis and an internal cohort. Despite resistance to immunotherapy, the high-risk group showed sensitivity to molecular targeted agents directed at IGF-1R (BMS-754807) and the PI3K-mTOR pathways (AZD8186, AZD8055). We experimentally validated these promising drugs for their inhibitory effects on MKN45 and MKN28 gastric cells. This study unveils the intricate interplay between TME and metabolic pathways in gastric cancer, offering potential for enhanced diagnosis, patient stratification, and personalized treatment. Understanding molecular features in each subtype enriches our comprehension of gastric cancer heterogeneity and potential therapeutic targets.
Keywords: M2 macrophage; cancer metabolism; gastric cancer; single-cell analysis; tumor microenvironment.
Copyright © 2024 Lin, Yang, Wang, Huang, Wang, Chen, Xu, Cai, Khan, Liu and Lin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Identification of cuproptosis-related subtypes, construction of a prognosis model, and tumor microenvironment landscape in gastric cancer.Front Immunol. 2022 Nov 21;13:1056932. doi: 10.3389/fimmu.2022.1056932. eCollection 2022. Front Immunol. 2022. PMID: 36479114 Free PMC article.
-
Revealing the crosstalk between LOX+ fibroblast and M2 macrophage in gastric cancer by single-cell sequencing.BMC Cancer. 2024 Sep 9;24(1):1117. doi: 10.1186/s12885-024-12861-y. BMC Cancer. 2024. PMID: 39251966 Free PMC article.
-
Identification of Cuproptosis-Related Subtypes, Establishment of a Prognostic Signature and Characterization of the Tumor Microenvironment in Gastric Cancer.Int J Gen Med. 2023 May 2;16:1631-1652. doi: 10.2147/IJGM.S404847. eCollection 2023. Int J Gen Med. 2023. PMID: 37168531 Free PMC article.
-
A novel necroptosis-related gene index for predicting prognosis and a cold tumor immune microenvironment in stomach adenocarcinoma.Front Immunol. 2022 Oct 27;13:968165. doi: 10.3389/fimmu.2022.968165. eCollection 2022. Front Immunol. 2022. PMID: 36389725 Free PMC article. Review.
-
Single-cell RNA sequencing in ovarian cancer: revealing new perspectives in the tumor microenvironment.Am J Transl Res. 2024 Jul 15;16(7):3338-3354. doi: 10.62347/SMSG9047. eCollection 2024. Am J Transl Res. 2024. PMID: 39114691 Free PMC article. Review.
Cited by
-
Integrative single-cell and multi-omics analyses reveal ferroptosis-associated gene expression and immune microenvironment heterogeneity in gastric cancer.Discov Oncol. 2025 Jan 17;16(1):57. doi: 10.1007/s12672-025-01798-8. Discov Oncol. 2025. PMID: 39831925 Free PMC article.
-
A Prognostic Riskscore Model Related to Helicobacter pylori Infection in Stomach Adenocarcinoma.Int J Genomics. 2025 Jan 21;2025:5554610. doi: 10.1155/ijog/5554610. eCollection 2025. Int J Genomics. 2025. PMID: 39886652 Free PMC article.
-
Tumor energy metabolism: implications for therapeutic targets.Mol Biomed. 2024 Nov 29;5(1):63. doi: 10.1186/s43556-024-00229-4. Mol Biomed. 2024. PMID: 39609317 Free PMC article. Review.
-
Multiple programmed cell death patterns predict the prognosis and drug sensitivity in gastric cancer.Front Immunol. 2025 Feb 4;16:1511453. doi: 10.3389/fimmu.2025.1511453. eCollection 2025. Front Immunol. 2025. PMID: 39967665 Free PMC article.
-
Single-cell Atlas reveals core function of CPVL/MSR1 expressing macrophages in the prognosis of triple-negative breast cancer.Front Immunol. 2024 Dec 24;15:1501009. doi: 10.3389/fimmu.2024.1501009. eCollection 2024. Front Immunol. 2024. PMID: 39776914 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous