

Association of Different Anticoagulation Strategies With Outcomes in Patients Hospitalized With Acute Pulmonary Embolism
- PMID: 38962644
- PMCID: PMC11219246
- DOI: 10.7759/cureus.61545
Association of Different Anticoagulation Strategies With Outcomes in Patients Hospitalized With Acute Pulmonary Embolism
Abstract
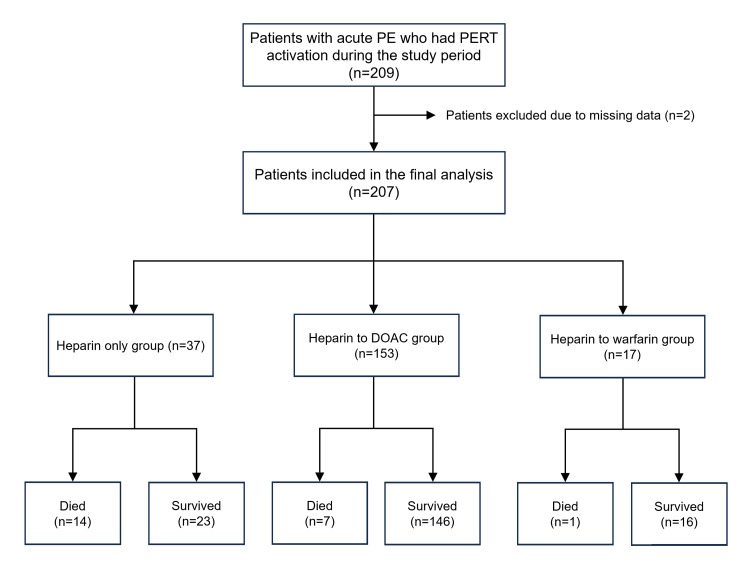
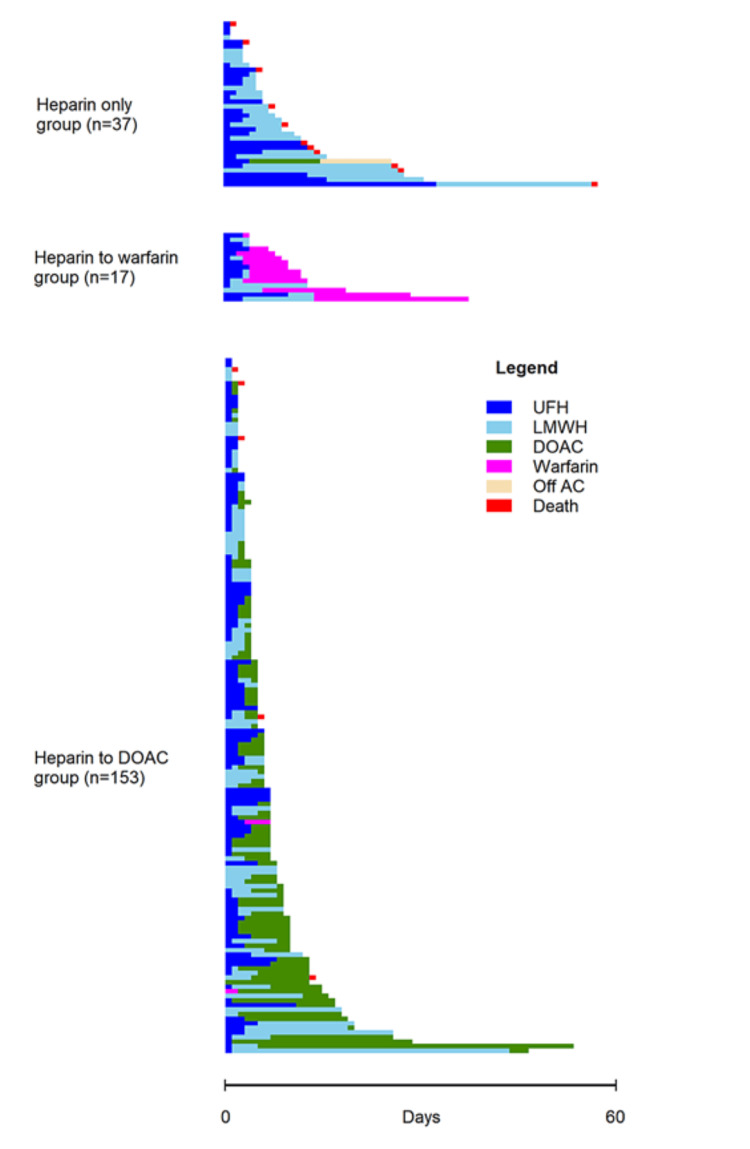
Background Therapeutic anticoagulation is the cornerstone of treatment for pulmonary embolism (PE), but the impact of different anticoagulation strategies on patient outcomes remains unclear. In this study, we assessed the association of different anticoagulation strategies with the outcomes of patients with acute PE. Methods A retrospective chart review of 207 patients with acute PE who were admitted to one of three urban teaching hospitals in the Mount Sinai Health System (in New York City) from January 2020 to September 2022 was performed. Demographic, clinical, and radiographic data were recorded for all patients. Multivariate regression analyses were performed to assess the association of different outcomes with the approach of therapeutic anticoagulation used. Results The median age of the included patients was 65 years, and 50.2% were women. The most common approach (n = 153, 73.9%) to therapeutic anticoagulation was initial treatment with unfractionated or low molecular weight heparin followed by a direct-acting oral anticoagulant (DOAC), while heparin alone (either unfractionated or low molecular weight heparin) was used in 37 (17.9%) patients, and another 17 (8.2%) patients were treated with heparin followed by bridging to warfarin. Hospital length of stay was longer for patients in the "heparin to warfarin" group (risk-adjusted incidence rate ratio of 2.52). The rates of in-hospital bleeding, all-cause 30-day mortality, and all-cause 30-day re-admissions did not have any significant association with the therapeutic anticoagulation approach used. Conclusion Patients with acute PE who were initially treated with heparin and subsequently bridged to warfarin had a longer hospital stay. Rates of in-hospital bleeding, 30-day mortality, and 30-day re-admission were not associated with the strategy of therapeutic anticoagulation employed.
Keywords: acute pulmonary embolism; anticoagulation bridge therapy; hemorrhage; length of hospital stay; mortality.
Copyright © 2024, Rehman et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Mount Sinai Institutional Review Board issued approval N/A. This retrospective observational study was approved by the institutional IRB at Mount Sinai-Icahn School of Medicine. As we only analyzed de-identified and anonymized data, and no actual patient contact was involved, the requirement of informed consent was waived by the IRB. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Rivaroxaban versus Heparin Bridging to Warfarin Therapy: Impact on Hospital Length of Stay and Treatment Costs for Low-Risk Patients with Pulmonary Embolism.Pharmacotherapy. 2016 Oct;36(10):1109-1115. doi: 10.1002/phar.1828. Epub 2016 Sep 19. Pharmacotherapy. 2016. PMID: 27548074
-
Anti-factor Xa as the preferred assay to monitor heparin for the treatment of pulmonary embolism.Int J Lab Hematol. 2024 Apr;46(2):354-361. doi: 10.1111/ijlh.14207. Epub 2023 Nov 21. Int J Lab Hematol. 2024. PMID: 37989523
-
Unsolved issues in the treatment of pulmonary embolism.Thromb Res. 2001 Sep 15;103(6):V245-55. doi: 10.1016/s0049-3848(01)00325-5. Thromb Res. 2001. PMID: 11567662 Review.
-
Evaluation of Time to Therapeutic Anticoagulation and Associated Outcomes in Critically Ill, Obese Patients With Pulmonary Embolism Receiving Unfractionated Heparin.J Pharm Pract. 2021 Jun;34(3):438-444. doi: 10.1177/0897190019878073. Epub 2019 Sep 29. J Pharm Pract. 2021. PMID: 31564199
-
Initial anticoagulation in patients with pulmonary embolism: thrombolysis, unfractionated heparin, LMWH, fondaparinux, or DOACs?Br J Clin Pharmacol. 2017 Nov;83(11):2356-2366. doi: 10.1111/bcp.13340. Epub 2017 Jul 9. Br J Clin Pharmacol. 2017. PMID: 28593681 Free PMC article. Review.
Cited by
-
Association of transfer time and delays with outcomes for patients with acute pulmonary embolism requiring interhospital transfer: a retrospective observational study.Ann Med. 2025 Dec;57(1):2534094. doi: 10.1080/07853890.2025.2534094. Epub 2025 Jul 25. Ann Med. 2025. PMID: 40711763 Free PMC article.
-
[Diagnosis and Treatment of Pulmonary Embolism and Pulmonary Hypertension in Patients With Interstitial Lung Disease].Open Respir Arch. 2025 Feb 6;7(1):100406. doi: 10.1016/j.opresp.2025.100406. eCollection 2025 Jan-Mar. Open Respir Arch. 2025. PMID: 40104013 Free PMC article. Review. Spanish.
References
-
- Acute pulmonary embolism. Stein PD, Matta F. Curr Probl Cardiol. 2010;35:314–376. - PubMed
-
- Epidemiology and incidence: the scope of the problem and risk factors for development of venous thromboembolism. Stein PD, Matta F. Crit Care Clin. 2011;27:907-32, vii. - PubMed
-
- Contemporary national trends and outcomes of pulmonary embolism in the United States. Sedhom R, Megaly M, Elbadawi A, et al. Am J Cardiol. 2022;176:132–138. - PubMed
-
- Economic burden of venous thromboembolism in hospitalized patients. Dobesh PP. Pharmacotherapy. 2009;29:943–953. - PubMed
-
- Outpatient treatment of low-risk pulmonary embolism in the era of direct oral anticoagulants: a systematic review. Maughan BC, Frueh L, McDonagh MS, Casciere B, Kline JA. Acad Emerg Med. 2021;28:226–239. - PubMed
LinkOut - more resources
Full Text Sources