

The Occurrence of Dropped Head Syndrome After a Cervical Medial Branch Nerve Block in a Patient With Cervicothoracic Kyphotic Deformity: A Case Report
- PMID: 38962649
- PMCID: PMC11221394
- DOI: 10.7759/cureus.61586
The Occurrence of Dropped Head Syndrome After a Cervical Medial Branch Nerve Block in a Patient With Cervicothoracic Kyphotic Deformity: A Case Report
Abstract
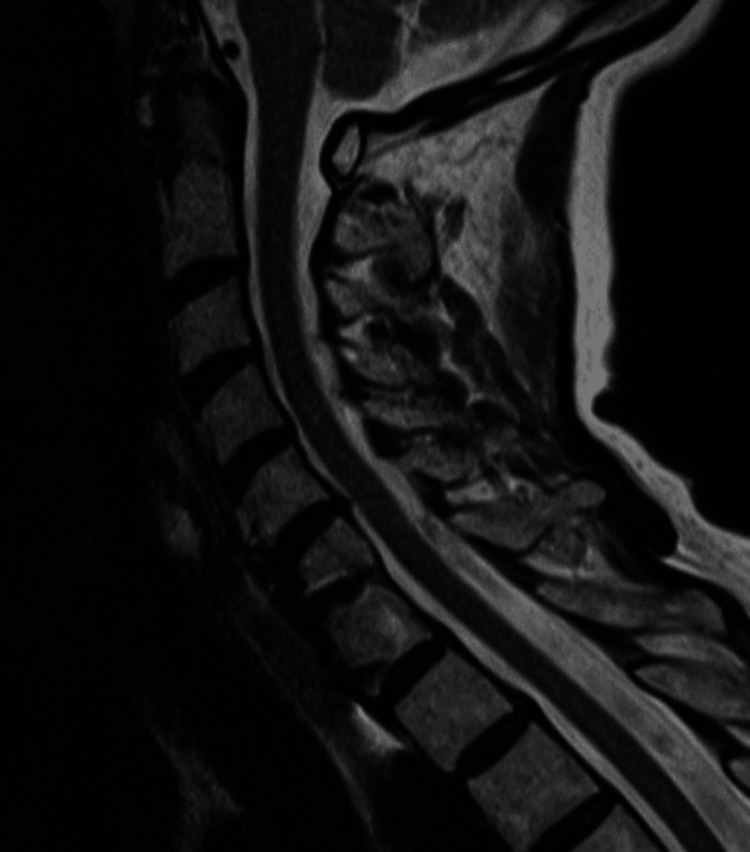
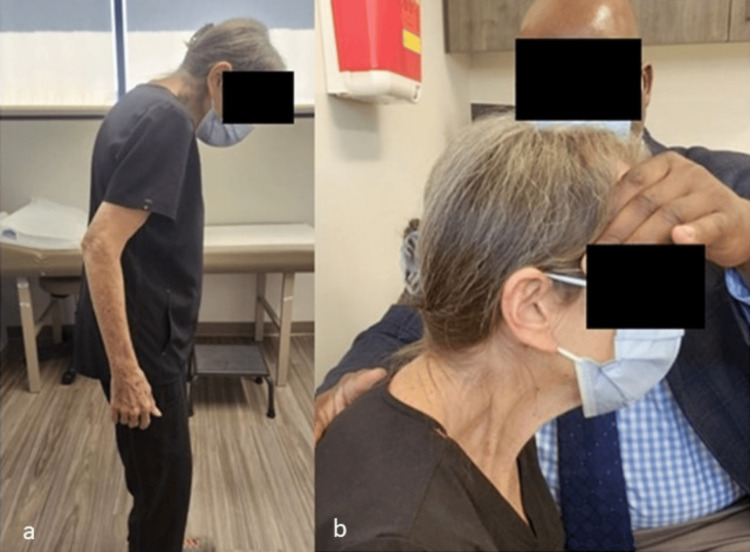
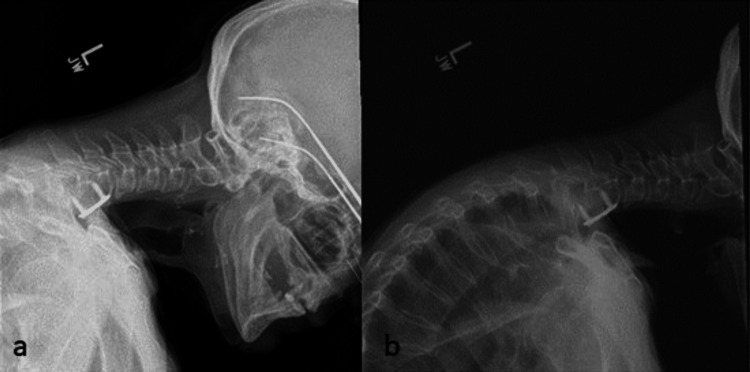
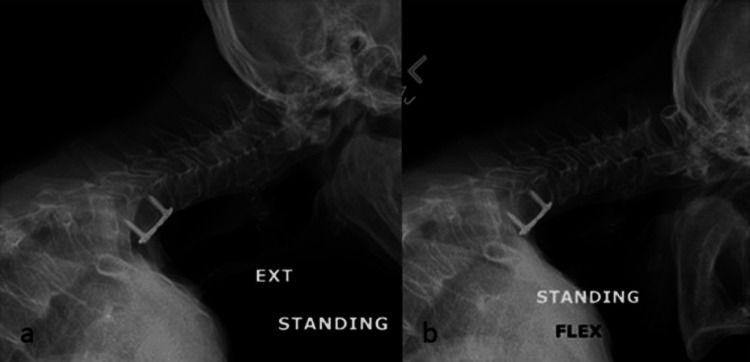
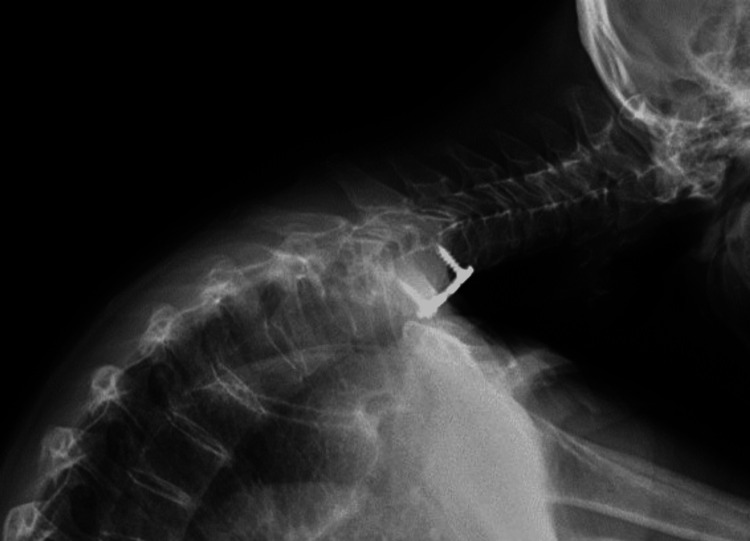
Complications from medial branch blocks (MBBs) are rare when following proper procedural protocol. Dropped head syndrome (DHS) is characterized by profound muscle weakness in the cervical spine, resulting in a failure to maintain a level horizontal gaze and, in the worst cases, a chin-on-chest deformity. In this case report, we described DHS developing after cervical MBBs using short-acting anesthetic agents and subsequent management. A 69-year-old woman with a previous C6-C7 anterior cervical discectomy and fusion (ACDF) underwent bilateral posterior cervical MBBs targeting the C4-C5 and C5-C6 levels. Immediately following the injection, she reported a sudden inability to lift her head and was subsequently diagnosed with DHS. This condition continued with minimal improvement for over six months. After weighing the risks, the patient elected to avoid surgery, and she was provided a soft cervical collar and prescribed physical therapy. DHS is a debilitating condition more commonly associated with neurodegenerative conditions and inflammatory myopathy, which has received limited attention due to its rarity as a complication of cervical radiofrequency neurotomy. Surgery for this condition, when considered, typically involves long-segment posterior cervical instrumented fusion. Undergoing such a surgery is a complicated discussion that should consider patient clinical factors and preferences. The clinical impact of loss of strength in paraspinal musculature in this patient population is clearly deserving of further study.
Keywords: cervical spine; deformity; dropped head syndrome; kyphosis; medial branch nerve block.
Copyright © 2024, Adeniran et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: Donna D. Ohnmeiss declare(s) support for attending board meetings from North American Spine Society Board of Directors. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Pediatric cervical kyphosis in the MRI era (1984-2008) with long-term follow up: literature review.Childs Nerv Syst. 2022 Feb;38(2):361-377. doi: 10.1007/s00381-021-05409-z. Epub 2021 Nov 22. Childs Nerv Syst. 2022. PMID: 34806157 Review.
-
Dropped head syndrome: report of a rare complication after multilevel bilateral cervical radiofrequency neurotomy.Pain Rep. 2022 Sep 14;7(5):e1037. doi: 10.1097/PR9.0000000000001037. eCollection 2022 Sep-Oct. Pain Rep. 2022. PMID: 36128045 Free PMC article.
-
Cervical Muscle Composition in Degenerative Dropped Head Syndrome: A Propensity Score Matching Study.Spine (Phila Pa 1976). 2025 Jun 13. doi: 10.1097/BRS.0000000000005424. Online ahead of print. Spine (Phila Pa 1976). 2025. PMID: 40509854
-
Catastrophic Dropped Head Syndrome Requiring Multiple Reconstruction Surgeries after Cervical Laminoplasty.Spine Surg Relat Res. 2018 Apr 7;2(3):243-247. doi: 10.22603/ssrr.2017-0084. eCollection 2018. Spine Surg Relat Res. 2018. PMID: 31440676 Free PMC article.
-
Surgical management of dropped head syndrome: A systematic review.Surg Neurol Int. 2022 Jun 17;13:255. doi: 10.25259/SNI_456_2022. eCollection 2022. Surg Neurol Int. 2022. PMID: 35855142 Free PMC article. Review.
References
-
- The annual incidence and course of neck pain in the general population: a population-based cohort study. Côté P, Cassidy DJ, Carroll LJ, Kristman V. Pain. 2004;112:267–273. - PubMed
-
- The prevalence of cervical zygapophyseal joint pain. A first approximation. Aprill C, Bogduk N. Spine (Phila Pa 1976) 1992;17:744–747. - PubMed
-
- Percutaneous radio-frequency neurotomy for chronic cervical zygapophyseal-joint pain. Lord SM, Barnsley L, Wallis BJ, McDonald GJ, Bogduk N. N Engl J Med. 1996;335:1721–1726. - PubMed
-
- Pulsed radiofrequency application in treatment of chronic zygapophyseal joint pain. Mikeladze G, Espinal R, Finnegan R, Routon J, Martin D. Spine J. 2003;3:360–362. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous