

Racial disparities in colorectal cancer outcomes and access to care: a multi-cohort analysis
- PMID: 38962767
- PMCID: PMC11220245
- DOI: 10.3389/fpubh.2024.1414361
Racial disparities in colorectal cancer outcomes and access to care: a multi-cohort analysis
Abstract
Introduction: Non-Hispanic Black (NHB) Americans have a higher incidence of colorectal cancer (CRC) and worse survival than non-Hispanic white (NHW) Americans, but the relative contributions of biological versus access to care remain poorly characterized. This study used two nationwide cohorts in different healthcare contexts to study health system effects on this disparity.
Methods: We used data from the Surveillance, Epidemiology, and End Results (SEER) registry as well as the United States Veterans Health Administration (VA) to identify adults diagnosed with colorectal cancer between 2010 and 2020 who identified as non-Hispanic Black (NHB) or non-Hispanic white (NHW). Stratified survival analyses were performed using a primary endpoint of overall survival, and sensitivity analyses were performed using cancer-specific survival.
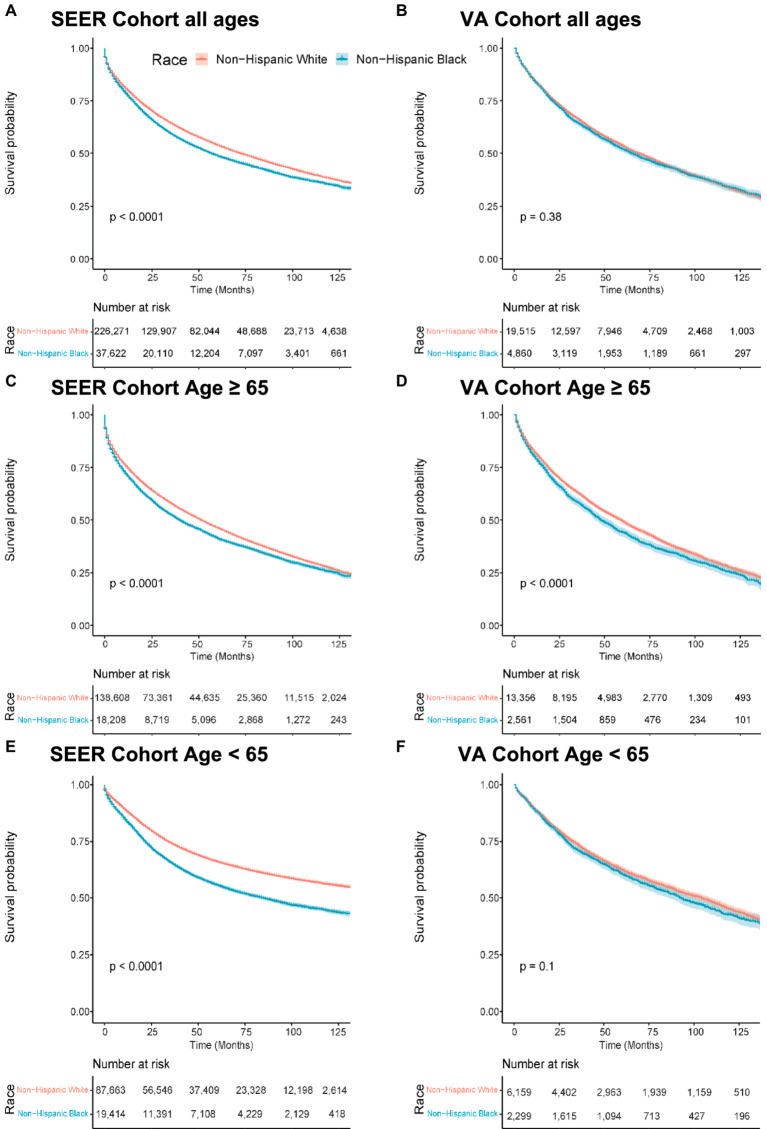
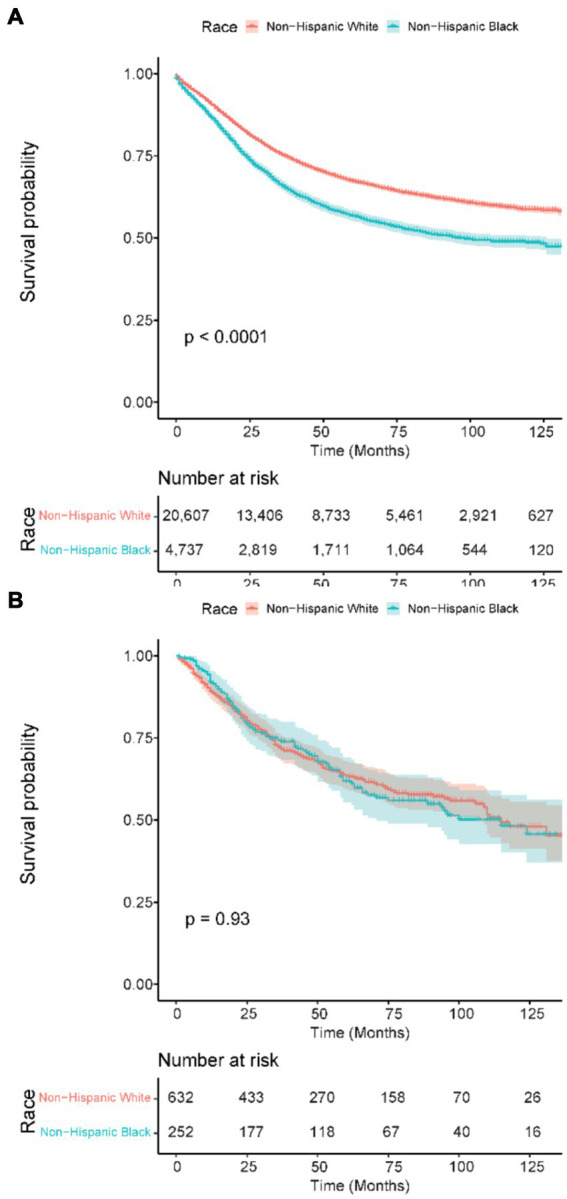
Results: We identified 263,893 CRC patients in the SEER registry (36,662 (14%) NHB; 226,271 (86%) NHW) and 24,375 VA patients (4,860 (20%) NHB; 19,515 (80%) NHW). In the SEER registry, NHB patients had worse OS than NHW patients: median OS of 57 months (95% confidence interval (CI) 55-58) versus 72 months (95% CI 71-73) (hazard ratio (HR) 1.14, 95% CI 1.12-1.15, p = 0.001). In contrast, VA NHB median OS was 65 months (95% CI 62-69) versus NHW 69 months (95% CI 97-71) (HR 1.02, 95% CI 0.98-1.07, p = 0.375). There was significant interaction in the SEER registry between race and Medicare age eligibility (p < 0.001); NHB race had more effect in patients <65 years old (HR 1.44, 95% CI 1.39-1.49, p < 0.001) than in those ≥65 (HR 1.13, 95% CI 1.11-1.15, p < 0.001). In the VA, age stratification was not significant (p = 0.21).
Discussion: Racial disparities in CRC survival in the general US population are significantly attenuated in Medicare-aged patients. This pattern is not present in the VA, suggesting that access to care may be an important component of racial disparities in this disease.
Keywords: colorectal cancer; disparities; health services research; outcomes; race; veteran affairs.
Copyright © 2024 Riviere, Morgan, Deshler, Demb, Mehtsun, Martinez, Gupta, Banegas, Murphy and Rose.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Patient-Physician Communication Experience Modifies Racial/Ethnic Health Care Disparities Among Surveillance, Epidemiology, and End Results-Consumer Assessment of Healthcare Providers and Systems Participants With Colorectal Cancer and Multiple Chronic Conditions.Med Care. 2025 Mar 1;63(3):256-265. doi: 10.1097/MLR.0000000000002112. Epub 2024 Dec 27. Med Care. 2025. PMID: 39739589
-
Racial and Ethnic Disparity for Cancer Mortality in General and Single-Payer Healthcare Systems in the United States.J Racial Ethn Health Disparities. 2025 Aug;12(4):2646-2654. doi: 10.1007/s40615-024-02077-y. Epub 2024 Jul 2. J Racial Ethn Health Disparities. 2025. PMID: 38955957 Free PMC article.
-
Racial/ethnic disparities in early-onset colorectal cancer: implications for a racial/ethnic-specific screening strategy.Cancer Med. 2021 Mar;10(6):2080-2087. doi: 10.1002/cam4.3811. Epub 2021 Feb 28. Cancer Med. 2021. PMID: 33641251 Free PMC article.
-
Mortality Disparities in Racial/Ethnic Minority Groups in the Veterans Health Administration: An Evidence Review and Map.Am J Public Health. 2018 Mar;108(3):e1-e11. doi: 10.2105/AJPH.2017.304246. Am J Public Health. 2018. PMID: 29412713 Free PMC article. Review.
-
African-American and Caucasian disparities in colorectal cancer mortality and survival by data source: an epidemiologic review.Cancer Biomark. 2007;3(6):301-13. doi: 10.3233/cbm-2007-3604. Cancer Biomark. 2007. PMID: 18048968 Free PMC article. Review.
Cited by
-
Multi-faceted strategies to advance health equity in colorectal cancer screening in primary care setting: quality improvement project.BMC Health Serv Res. 2024 Nov 18;24(1):1422. doi: 10.1186/s12913-024-11928-7. BMC Health Serv Res. 2024. PMID: 39558206 Free PMC article.
-
Counties with Low Employment and Education Status Are Associated with Higher Age-Adjusted Cancer Mortality.Cancers (Basel). 2025 Jun 19;17(12):2051. doi: 10.3390/cancers17122051. Cancers (Basel). 2025. PMID: 40563700 Free PMC article.