

Retroperitoneum revisited: a review of radiological literature and updated concept of retroperitoneal fascial anatomy with imaging features and correlating anatomy
- PMID: 38963431
- PMCID: PMC11246311
- DOI: 10.1007/s00276-024-03432-8
Retroperitoneum revisited: a review of radiological literature and updated concept of retroperitoneal fascial anatomy with imaging features and correlating anatomy
Abstract
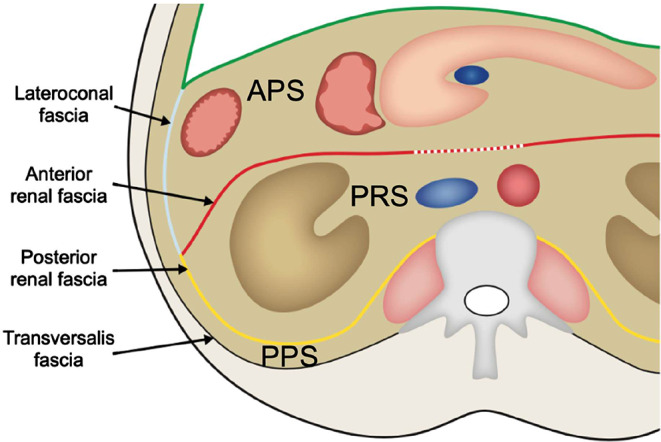
Purpose: Spread of disease in the retroperitoneum is dictated by the complex anatomy of retroperitoneal fasciae and is still incompletely understood. Conflicting reports have led to insufficient and incorrect anatomical concepts in radiological literature.
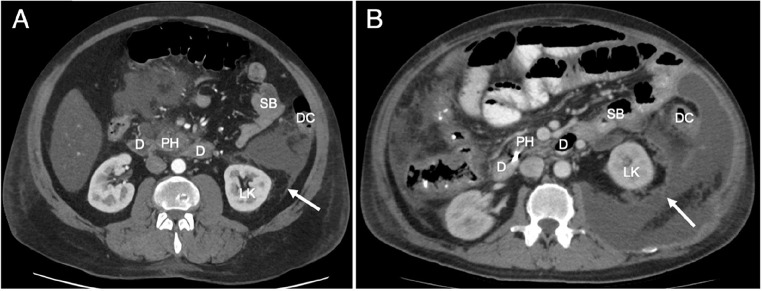
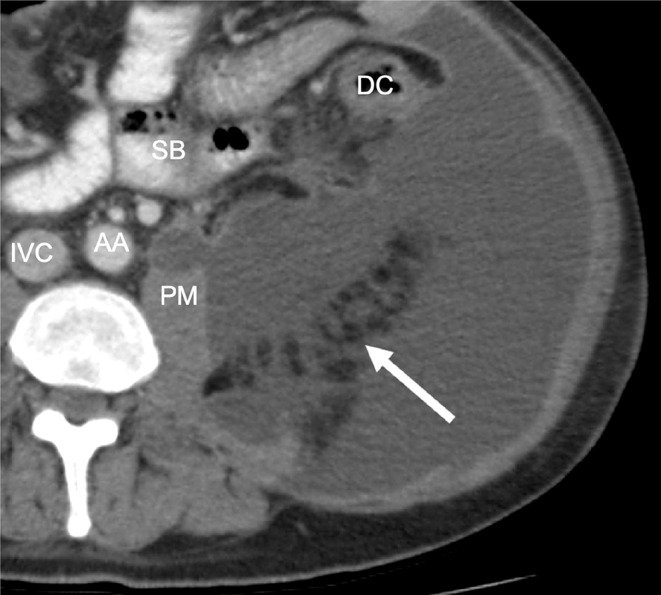
Methods: This review will discuss previous concepts prevalent in radiological literature and their shortcomings will be highlighted. New insights from recent anatomical and embryological research, together with imaging examples, will be used to clarify patterns of disease spread in the retroperitoneum that remain unexplained by these concepts.
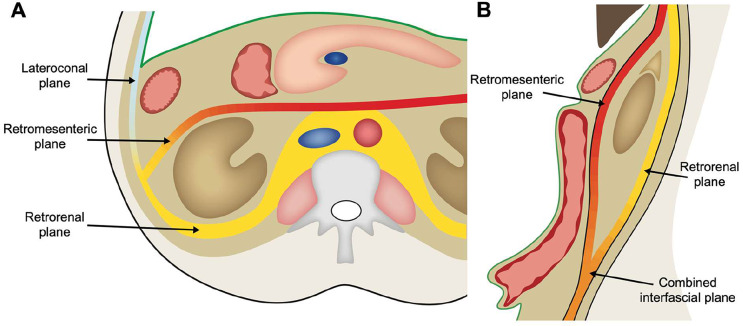
Results: The fusion fascia and the renal fascia in particular give rise to planes and spaces that act as vectors for spread of disease in the retroperitoneum. Some of these planes and structures, such as the caudal extension of the renal fascia, have previously not been described in radiological literature.
Conclusion: New insights, including the various fasciae, potential spaces and planes, are incorporated into an updated combined retroperitoneal fascial concept.
Keywords: Anatomy; Fascia; Imaging; Radiology; Retroperitoneum.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
