

Mitochondrial Structure and Function in Human Heart Failure
- PMID: 38963864
- PMCID: PMC11225798
- DOI: 10.1161/CIRCRESAHA.124.323800
Mitochondrial Structure and Function in Human Heart Failure
Abstract
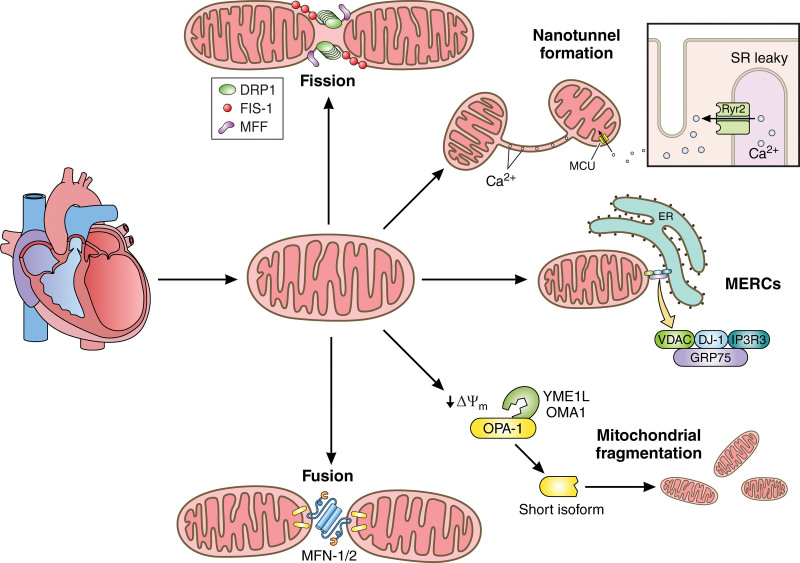
Despite clinical and scientific advancements, heart failure is the major cause of morbidity and mortality worldwide. Both mitochondrial dysfunction and inflammation contribute to the development and progression of heart failure. Although inflammation is crucial to reparative healing following acute cardiomyocyte injury, chronic inflammation damages the heart, impairs function, and decreases cardiac output. Mitochondria, which comprise one third of cardiomyocyte volume, may prove a potential therapeutic target for heart failure. Known primarily for energy production, mitochondria are also involved in other processes including calcium homeostasis and the regulation of cellular apoptosis. Mitochondrial function is closely related to morphology, which alters through mitochondrial dynamics, thus ensuring that the energy needs of the cell are met. However, in heart failure, changes in substrate use lead to mitochondrial dysfunction and impaired myocyte function. This review discusses mitochondrial and cristae dynamics, including the role of the mitochondria contact site and cristae organizing system complex in mitochondrial ultrastructure changes. Additionally, this review covers the role of mitochondria-endoplasmic reticulum contact sites, mitochondrial communication via nanotunnels, and altered metabolite production during heart failure. We highlight these often-neglected factors and promising clinical mitochondrial targets for heart failure.
Keywords: cardiovascular diseases; heart failure; hypertension; mitochondria; myocardium.
Conflict of interest statement
None.
Figures
Similar articles
-
Binding of FUN14 Domain Containing 1 With Inositol 1,4,5-Trisphosphate Receptor in Mitochondria-Associated Endoplasmic Reticulum Membranes Maintains Mitochondrial Dynamics and Function in Hearts in Vivo.Circulation. 2017 Dec 5;136(23):2248-2266. doi: 10.1161/CIRCULATIONAHA.117.030235. Epub 2017 Sep 23. Circulation. 2017. PMID: 28942427 Free PMC article.
-
The intestine responds to heart failure by enhanced mitochondrial fusion through glucagon-like peptide-1 signalling.Cardiovasc Res. 2019 Nov 1;115(13):1873-1885. doi: 10.1093/cvr/cvz002. Cardiovasc Res. 2019. PMID: 30629149
-
Reduced reticulum-mitochondria Ca2+ transfer is an early and reversible trigger of mitochondrial dysfunctions in diabetic cardiomyopathy.Basic Res Cardiol. 2020 Nov 30;115(6):74. doi: 10.1007/s00395-020-00835-7. Basic Res Cardiol. 2020. PMID: 33258101 Free PMC article.
-
Mitochondrial Dysfunction and Heart Disease: Critical Appraisal of an Overlooked Association.Int J Mol Sci. 2021 Jan 9;22(2):614. doi: 10.3390/ijms22020614. Int J Mol Sci. 2021. PMID: 33435429 Free PMC article. Review.
-
Mitochondrial Bioenergetics and Dysfunction in Failing Heart.Adv Exp Med Biol. 2017;982:65-80. doi: 10.1007/978-3-319-55330-6_4. Adv Exp Med Biol. 2017. PMID: 28551782 Review.
Cited by
-
Stellate Ganglia: A Key Therapeutic Target for Malignant Ventricular Arrhythmia in Heart Disease.Circ Res. 2025 Apr 25;136(9):1049-1069. doi: 10.1161/CIRCRESAHA.124.325384. Epub 2025 Apr 24. Circ Res. 2025. PMID: 40273204 Review.
-
Cardiac MRI Strain as an Early Indicator of Myocardial Dysfunction in Hypertrophic Cardiomyopathy.Int J Mol Sci. 2025 Feb 7;26(4):1407. doi: 10.3390/ijms26041407. Int J Mol Sci. 2025. PMID: 40003877 Free PMC article.
-
SIRT6 mitigates doxorubicin-induced cardiomyopathy via amelioration of mitochondrial dysfunction: A mechanistic study implicating the activation of the Nrf-2/FUNDC1 signaling axis.Int J Med Sci. 2025 Feb 28;22(7):1640-1657. doi: 10.7150/ijms.101520. eCollection 2025. Int J Med Sci. 2025. PMID: 40093797 Free PMC article.
-
Expert Consensus on the Diagnosis and Management of Carotid Atherosclerotic Plaque: Pathophysiology, Clinical Management, and Preventive Approaches.Int J Med Sci. 2025 May 30;22(11):2738-2756. doi: 10.7150/ijms.107479. eCollection 2025. Int J Med Sci. 2025. PMID: 40520900 Free PMC article. Review.
-
Accuracy and reliability of non-invasive pressure-strain loop for myocardial work assessment in functional single ventricle patients.BMC Cardiovasc Disord. 2025 Aug 2;25(1):575. doi: 10.1186/s12872-025-05017-8. BMC Cardiovasc Disord. 2025. PMID: 40753366 Free PMC article.
References
-
- Vaduganathan M, Mensah GA, Turco JV, Fuster V, Roth GA. The global burden of cardiovascular diseases and risk: a compass for future health. J Am Coll Cardiol. 2022;80:2361–2371. doi: 10.1016/j.jacc.2022.11.005 - PubMed
-
- Office of the Associate Director for Policy and Strategy. Health Topics: Heart Disease and Heart Attack. Centers for Disease Control and Prevention; 2021
-
- Haddad F, Hunt S, Rosenthal D, Murphy D. Right ventricular function in cardiovascular disease, Part I: anatomy, physiology, aging, and functional assessment of the right ventricle. Circulation. 2008;117:1436–1448. doi: 10.1161/CIRCULATIONAHA.107.653576 - PubMed
-
- Fox KF, Cowie MR, Wood DA, Coats AJS, Gibbs JSR, Underwood SR, Turner RM, Poole-Wilson PA, Davies SW, Sutton GC. Coronary artery disease as the cause of incident heart failure in the population. Eur Heart J. 2001;22:228–236. doi: 10.1053/euhj.2000.2289 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
