

Bronchoscopy with and without needle-based confocal laser endomicroscopy for peripheral lung nodule diagnosis: protocol for a multicentre randomised controlled trial (CLEVER trial)
- PMID: 38964802
- PMCID: PMC11227804
- DOI: 10.1136/bmjopen-2023-081148
Bronchoscopy with and without needle-based confocal laser endomicroscopy for peripheral lung nodule diagnosis: protocol for a multicentre randomised controlled trial (CLEVER trial)
Abstract
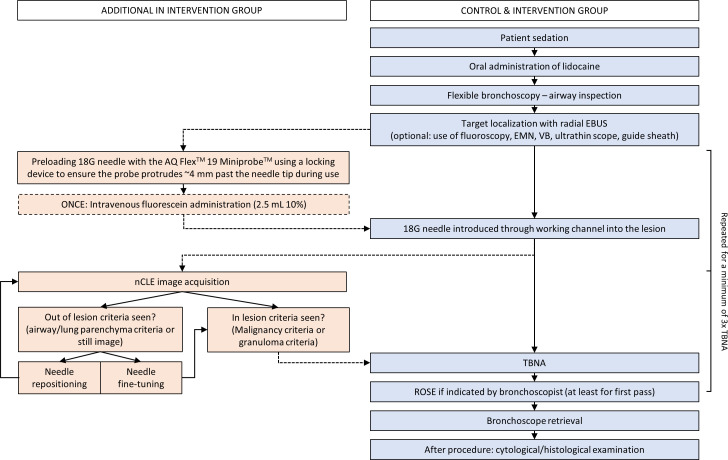
Introduction: Despite many technological advances, the diagnostic yield of bronchoscopic peripheral lung nodule analysis remains limited due to frequent mispositioning. Needle-based confocal laser endomicroscopy (nCLE) enables real-time microscopic feedback on needle positioning, potentially improving the sampling location and diagnostic yield. Previous studies have defined and validated nCLE criteria for malignancy, airway and lung parenchyma. Larger studies demonstrating the effect of nCLE on diagnostic yield are lacking. We aim to investigate if nCLE-imaging integrated with conventional bronchoscopy results in a higher diagnostic yield compared with conventional bronchoscopy without nCLE.
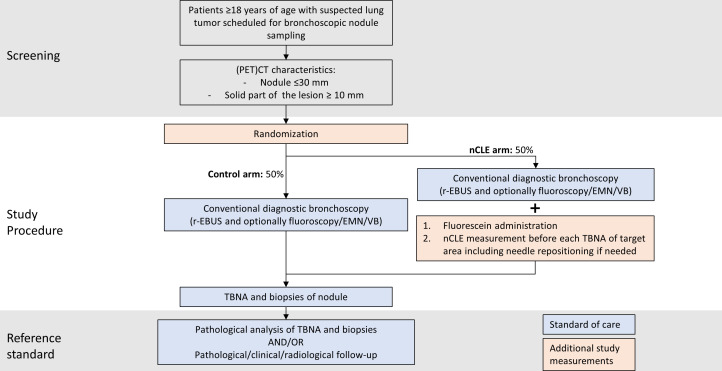
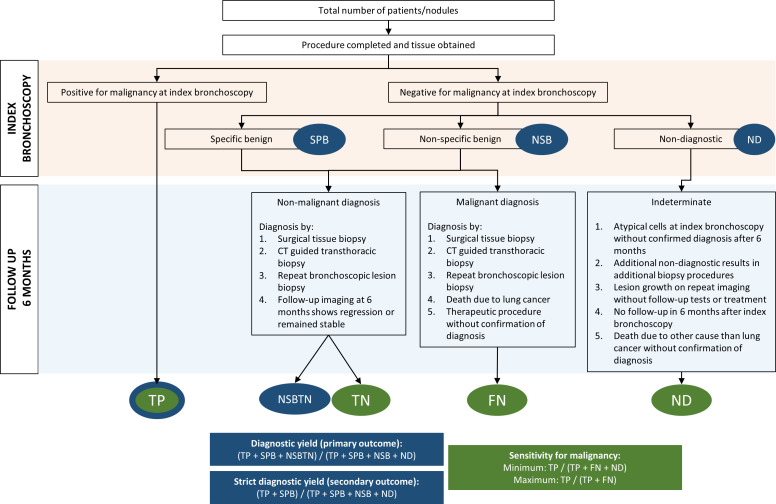
Methods and analysis: This is a parallel-group randomised controlled trial. Recruitment is performed at pulmonology outpatient clinics in universities and general hospitals in six different European countries and one hospital in the USA. Consecutive patients with a for malignancy suspected peripheral lung nodule (10-30 mm) with an indication for diagnostic bronchoscopy will be screened, and 208 patients will be included. Web-based randomisation (1:1) between the two procedures will be performed. The primary outcome is diagnostic yield. Secondary outcomes include diagnostic sensitivity for malignancy, needle repositionings, procedure and fluoroscopy duration, and complications. Pathologists will be blinded to procedure type; patients and endoscopists will not.
Ethics and dissemination: Primary approval by the Ethics Committee of the Amsterdam University Medical Center. Dissemination involves publication in a peer-reviewed journal.
Support: Financial and material support from Mauna Kea Technologies.
Trial registration number: NCT06079970.
Keywords: Biopsy; Clinical Trial; Cytopathology; Diagnostic Imaging; Respiratory tract tumours.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JTA declares material and financial support to the sponsor’s institution from Mauna Kea Technologies for this study. All Cellvizio equipment needed for the conduct of the study is provided in-kind to participating centers. All other authors declare no other conflicts of interest.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical