

Concomitant decrease of E- and A-FABP expression predicts worse survival in urothelial bladder cancer patients
- PMID: 38965292
- PMCID: PMC11224272
- DOI: 10.1038/s41598-024-65972-8
Concomitant decrease of E- and A-FABP expression predicts worse survival in urothelial bladder cancer patients
Abstract
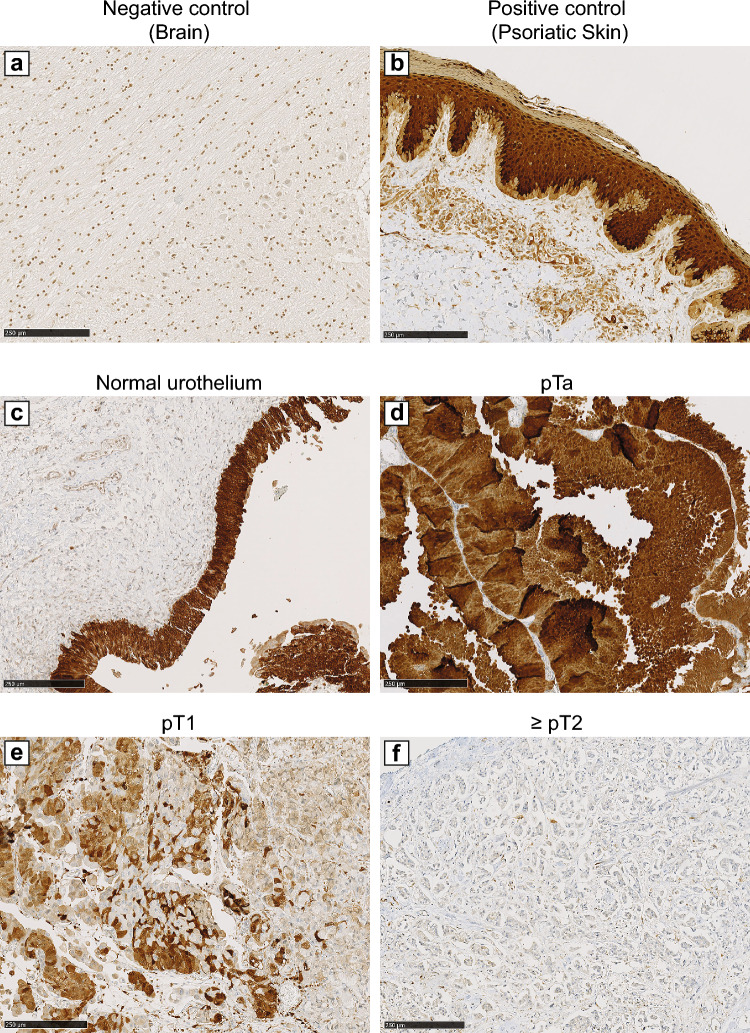
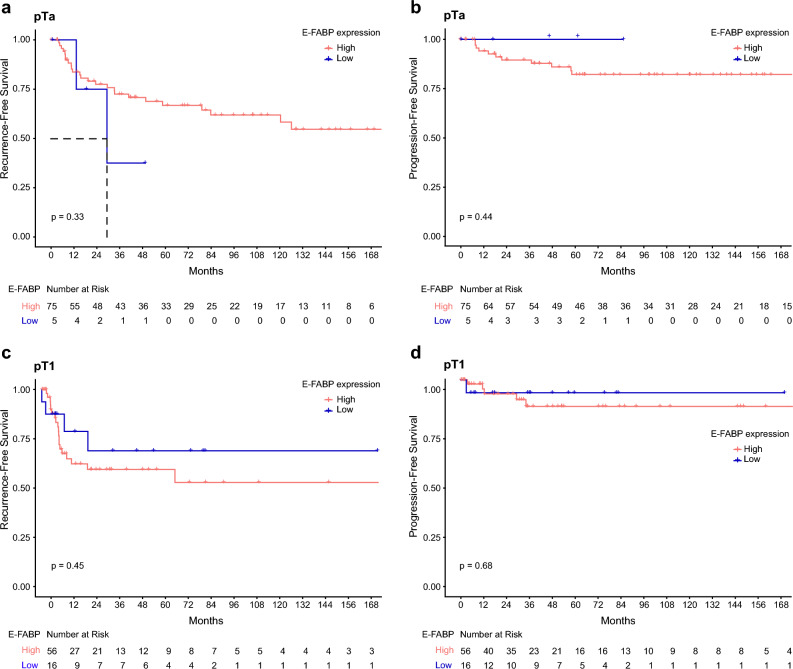
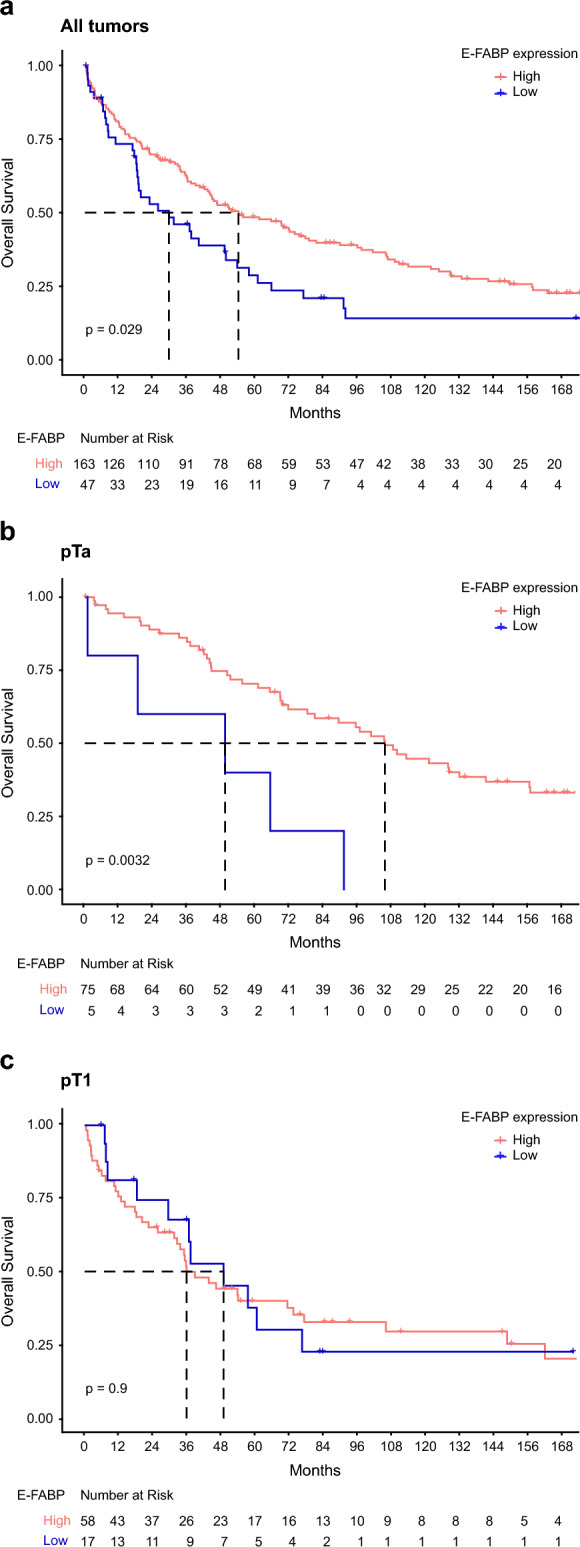
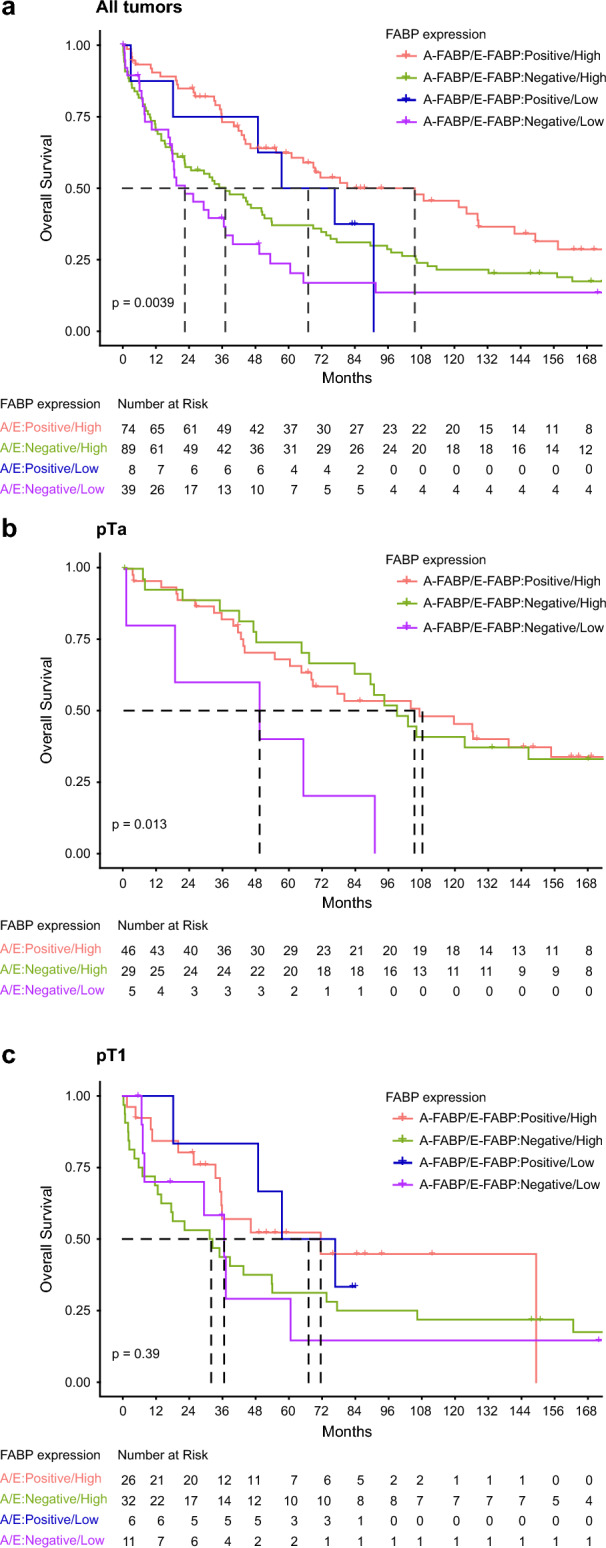
Non-muscle invasive bladder cancers (NMIBC) pTa-pT1 are depicted by a high risk of recurrence and/or progression with an unpredictable clinical evolution. Our aim was to identify, from the original resection specimen, tumors that will progress to better manage patients. We previously showed that A-FABP (Adipocyte- Fatty Acid Binding Protein) loss predicted NMIBC progression. Here we determined by immunohistochemistry the prognostic value of E-FABP (Epidermal-Fatty Acid Binding Protein) expression in 210 tumors (80 pTa, 75 pT1, 55 pT2-T4). Thus, E-FABP low expression was correlated with a high grade/stage, the presence of metastatic lymph nodes, and visceral metastases (p < 0.001). Unlike A-FABP in NMIBC, E-FABP low expression was not associated with RFS or PFS in Kaplan-Meier analysis. But patients of the overall cohort with a high E-FABP expression had a longer mOS (53.8 months vs. 29.3 months, p = 0.029). The immunohistochemical analysis on the same NMIBC tissue sections revealed that when A-FABP is absent, a high E-FABP expression is detected. E-FABP could compensate A-FABP loss. Interestingly, patients, whose original tumor presents both low E-FABP and negative A-FABP, had the worse survival, those maintaining the expression of both markers had better survival. To conclude, the combined evaluation of A- and E-FABP expression allowed to stratify patients with urothelial carcinoma for optimizing treatment and follow-up.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Gospodarowicz MK, Mason M. Urological Tumors. In: Brierley DJ, Gospodarowicz MK, Wittekind C, editors. TNM Classification of Malignant Tumors. 8. Wiley; 2017. pp. 204–207.
-
- Kurth KH, et al. Treatment of superficial bladder tumors: Achievements and needs. The EORTC Genitourinary Group. Eur Urol. 2000;37:1–9. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
