

AI-based differential diagnosis of dementia etiologies on multimodal data
- PMID: 38965435
- PMCID: PMC11485262
- DOI: 10.1038/s41591-024-03118-z
AI-based differential diagnosis of dementia etiologies on multimodal data
Abstract
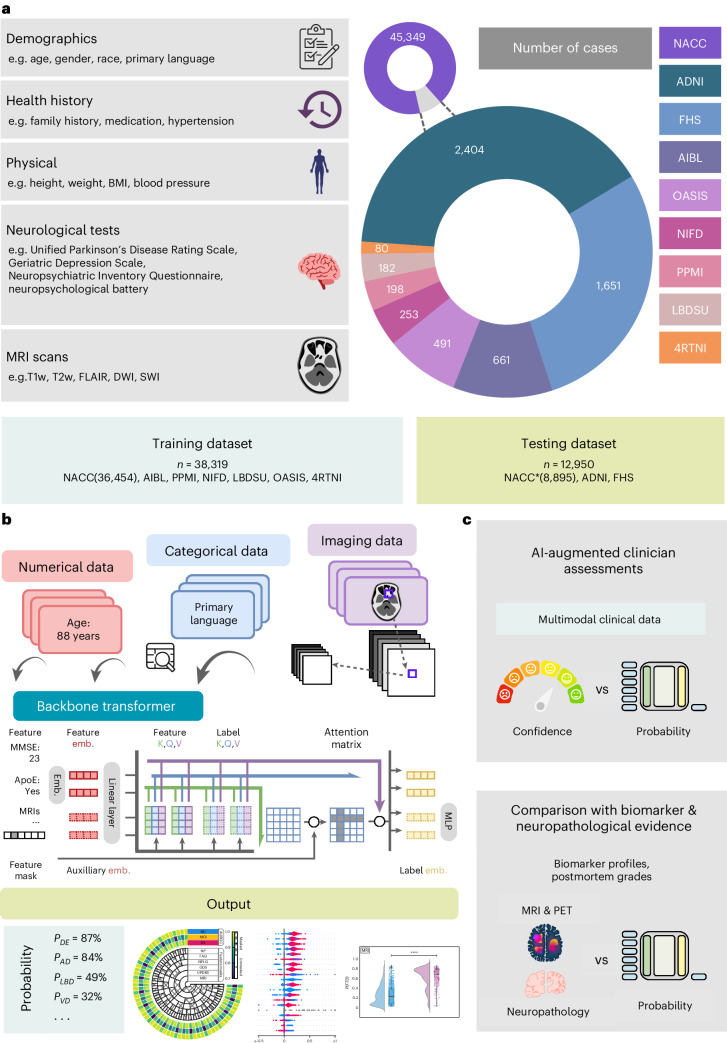
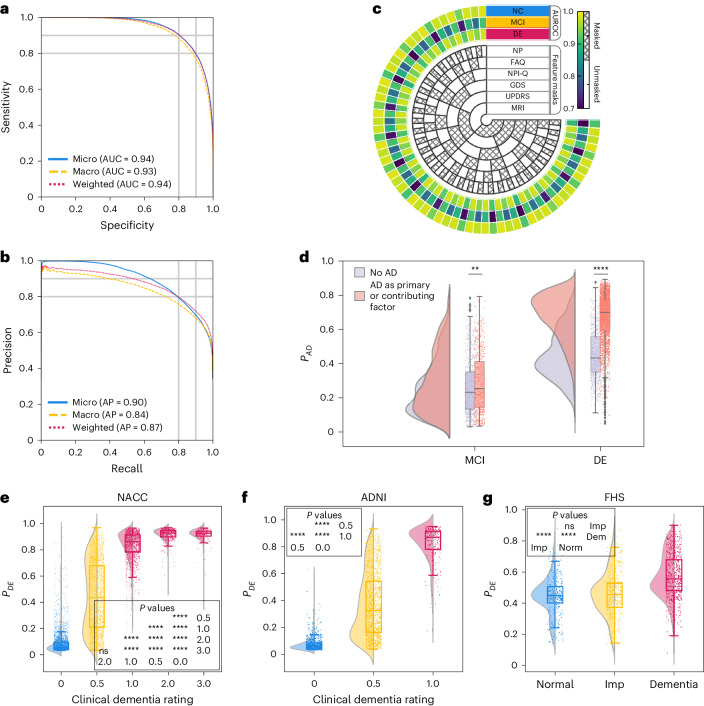
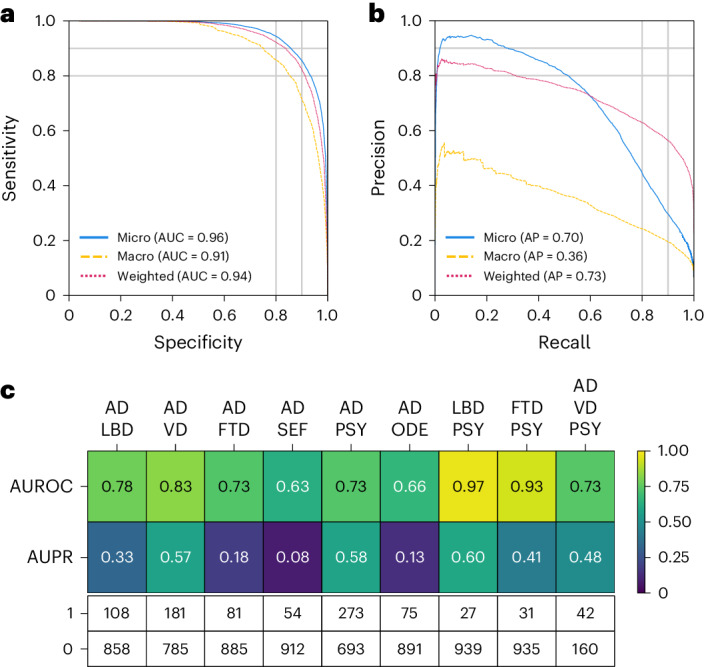
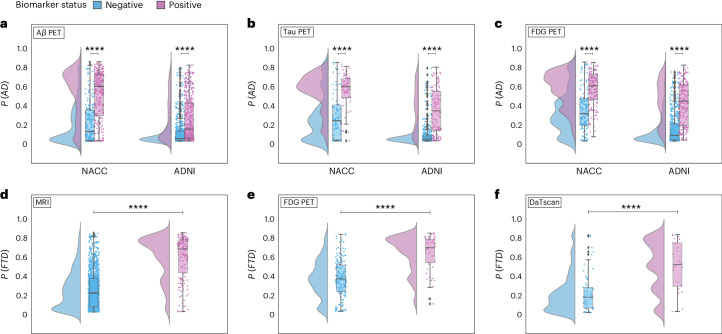
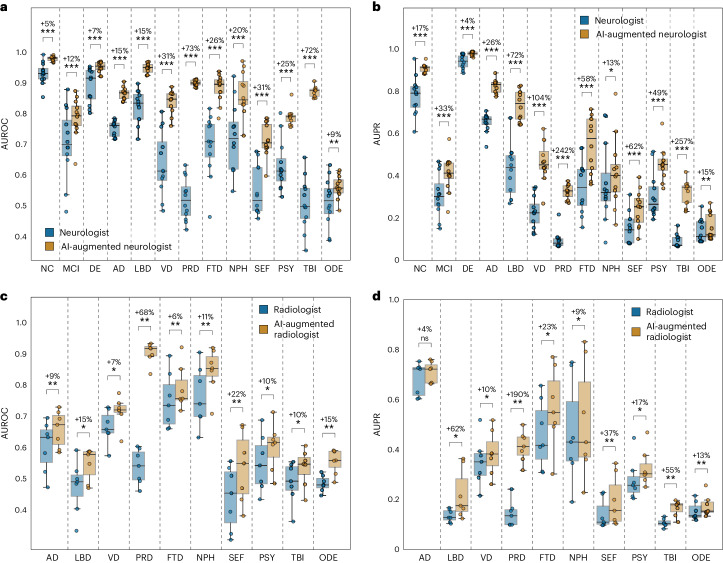
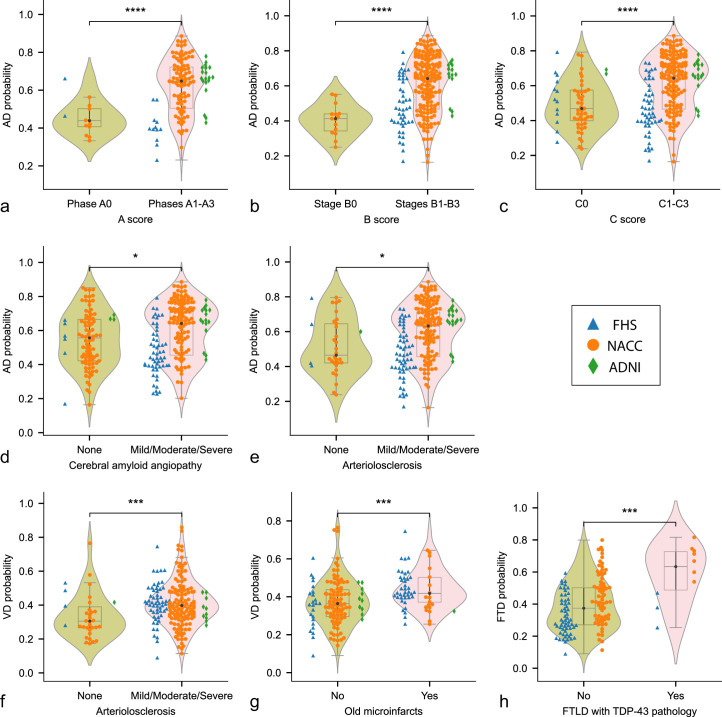
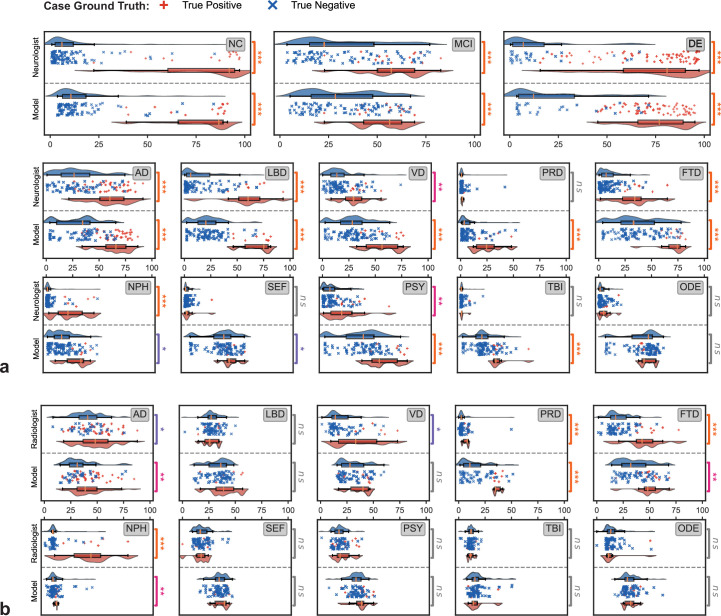
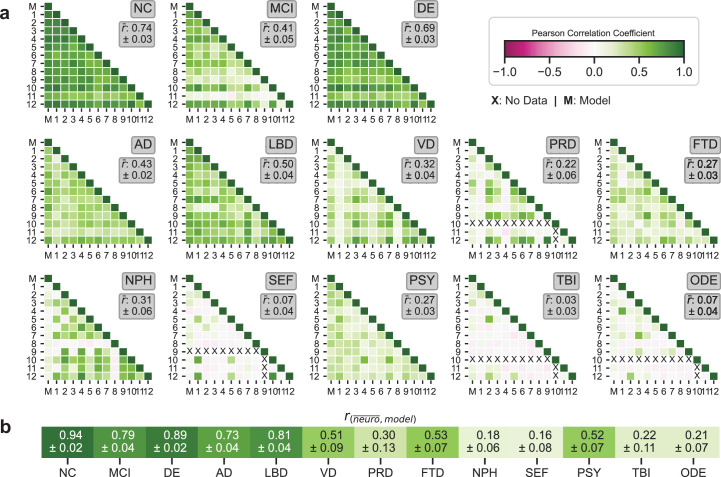
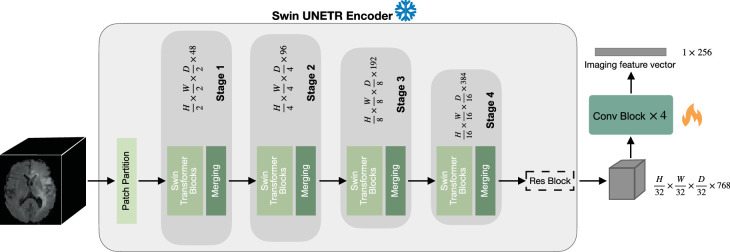
Differential diagnosis of dementia remains a challenge in neurology due to symptom overlap across etiologies, yet it is crucial for formulating early, personalized management strategies. Here, we present an artificial intelligence (AI) model that harnesses a broad array of data, including demographics, individual and family medical history, medication use, neuropsychological assessments, functional evaluations and multimodal neuroimaging, to identify the etiologies contributing to dementia in individuals. The study, drawing on 51,269 participants across 9 independent, geographically diverse datasets, facilitated the identification of 10 distinct dementia etiologies. It aligns diagnoses with similar management strategies, ensuring robust predictions even with incomplete data. Our model achieved a microaveraged area under the receiver operating characteristic curve (AUROC) of 0.94 in classifying individuals with normal cognition, mild cognitive impairment and dementia. Also, the microaveraged AUROC was 0.96 in differentiating the dementia etiologies. Our model demonstrated proficiency in addressing mixed dementia cases, with a mean AUROC of 0.78 for two co-occurring pathologies. In a randomly selected subset of 100 cases, the AUROC of neurologist assessments augmented by our AI model exceeded neurologist-only evaluations by 26.25%. Furthermore, our model predictions aligned with biomarker evidence and its associations with different proteinopathies were substantiated through postmortem findings. Our framework has the potential to be integrated as a screening tool for dementia in clinical settings and drug trials. Further prospective studies are needed to confirm its ability to improve patient care.
© 2024. The Author(s).
Conflict of interest statement
V.B.K. is on the scientific advisory board for Altoida Inc., and serves as a consultant to AstraZeneca. S.K. serves as consultant to AstraZeneca. C.W.F. is a consultant to Boston Imaging Core Lab. K.L.P. is a member of the scientific advisory boards for Curasen, Biohaven and Neuron23, receiving consulting fees and stock options, and for Amprion, receiving stock options. R.A. is a scientific advisor to Signant Health and NovoNordisk. She also serves as a consultant to Davos Alzheimer’s Collaborative. The remaining authors declare no competing interests.
Figures
Update of
-
AI-based differential diagnosis of dementia etiologies on multimodal data.medRxiv [Preprint]. 2024 Mar 26:2024.02.08.24302531. doi: 10.1101/2024.02.08.24302531. medRxiv. 2024. Update in: Nat Med. 2024 Oct;30(10):2977-2989. doi: 10.1038/s41591-024-03118-z. PMID: 38585870 Free PMC article. Updated. Preprint.
References
-
- World Health Organization. Global Status Report on the Public Health Response to Dementia: Web Annex Methodology for Producing Global Dementia Cost Estimates (World Health Organization, 2021). https://www.who.int/publications/i/item/9789240033245
-
- Cahill, S. Who’s global action plan on the public health response to dementia: some challenges and opportunities. Aging Ment. Health24, 197–199 (2019). - PubMed
-
- Gauthier, S. et al. Why has therapy development for dementia failed in the last two decades? Alzheimer Dement.12, 60–64 (2016). - PubMed
-
- Schneider, J. A., Arvanitakis, Z., Bang, W. & Bennett, D. A. Mixed brain pathologies account for most dementia cases in community-dwelling older persons. Neurology69, 2197–2204 (2007). - PubMed
MeSH terms
Grants and funding
- P20 AG068053/AG/NIA NIH HHS/United States
- P30 AG066515/AG/NIA NIH HHS/United States
- RF1 AG062109/AG/NIA NIH HHS/United States
- P30 AG066519/AG/NIA NIH HHS/United States
- P30 AG072973/AG/NIA NIH HHS/United States
- P30 AG066462/AG/NIA NIH HHS/United States
- P30 AG066530/AG/NIA NIH HHS/United States
- R01 HL159620/HL/NHLBI NIH HHS/United States
- P20 AG068077/AG/NIA NIH HHS/United States
- P30 AG072972/AG/NIA NIH HHS/United States
- P20 AG068082/AG/NIA NIH HHS/United States
- P30 AG072975/AG/NIA NIH HHS/United States
- P30 AG066444/AG/NIA NIH HHS/United States
- P30 AG066507/AG/NIA NIH HHS/United States
- P30 AG072946/AG/NIA NIH HHS/United States
- P30 AG066518/AG/NIA NIH HHS/United States
- P30 AG066511/AG/NIA NIH HHS/United States
- U24 AG072122/AG/NIA NIH HHS/United States
- P30 AG066512/AG/NIA NIH HHS/United States
- P30 AG062421/AG/NIA NIH HHS/United States
- U01 AG024904/AG/NIA NIH HHS/United States
- P30 AG066508/AG/NIA NIH HHS/United States
- P01 AG003991/AG/NIA NIH HHS/United States
- P30 AG072978/AG/NIA NIH HHS/United States
- P01 AG026276/AG/NIA NIH HHS/United States
- P30 AG062429/AG/NIA NIH HHS/United States
- P30 AG062422/AG/NIA NIH HHS/United States
- R01 AG079280/AG/NIA NIH HHS/United States
- P20 GM130447/GM/NIGMS NIH HHS/United States
- P30 AG066509/AG/NIA NIH HHS/United States
- P30 AG066546/AG/NIA NIH HHS/United States
- R43 DK134273/DK/NIDDK NIH HHS/United States
- K23 NS075097/NS/NINDS NIH HHS/United States
- R21 CA253498/CA/NCI NIH HHS/United States
- P30 AG072977/AG/NIA NIH HHS/United States
- P30 AG062677/AG/NIA NIH HHS/United States
- P50 AG047366/AG/NIA NIH HHS/United States
- P20 AG068024/AG/NIA NIH HHS/United States
- P30 AG072958/AG/NIA NIH HHS/United States
- P30 AG062715/AG/NIA NIH HHS/United States
- P30 AG066506/AG/NIA NIH HHS/United States
- P30 AG066468/AG/NIA NIH HHS/United States
- P30 AG072976/AG/NIA NIH HHS/United States
- P30 AG072947/AG/NIA NIH HHS/United States
- P30 AG072931/AG/NIA NIH HHS/United States
- P30 AG066514/AG/NIA NIH HHS/United States
- P30 AG072959/AG/NIA NIH HHS/United States
- U19 AG068753/AG/NIA NIH HHS/United States
- P30 AG072979/AG/NIA NIH HHS/United States
- R01 NS115114/NS/NINDS NIH HHS/United States
- UL1 TR001430/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
