

Comprehensive analysis and identification of subtypes and hub genes of high immune response in lung adenocarcinoma
- PMID: 38965571
- PMCID: PMC11225283
- DOI: 10.1186/s12890-024-03130-6
Comprehensive analysis and identification of subtypes and hub genes of high immune response in lung adenocarcinoma
Abstract
Background: The advent of immunotherapy targeting immune checkpoints has conferred significant clinical advantages to patients with lung adenocarcinoma (LUAD); However, only a limited subset of patients exhibit responsiveness to this treatment. Consequently, there is an imperative need to stratify LUAD patients based on their response to immunotherapy and enhance the therapeutic efficacy of these treatments.
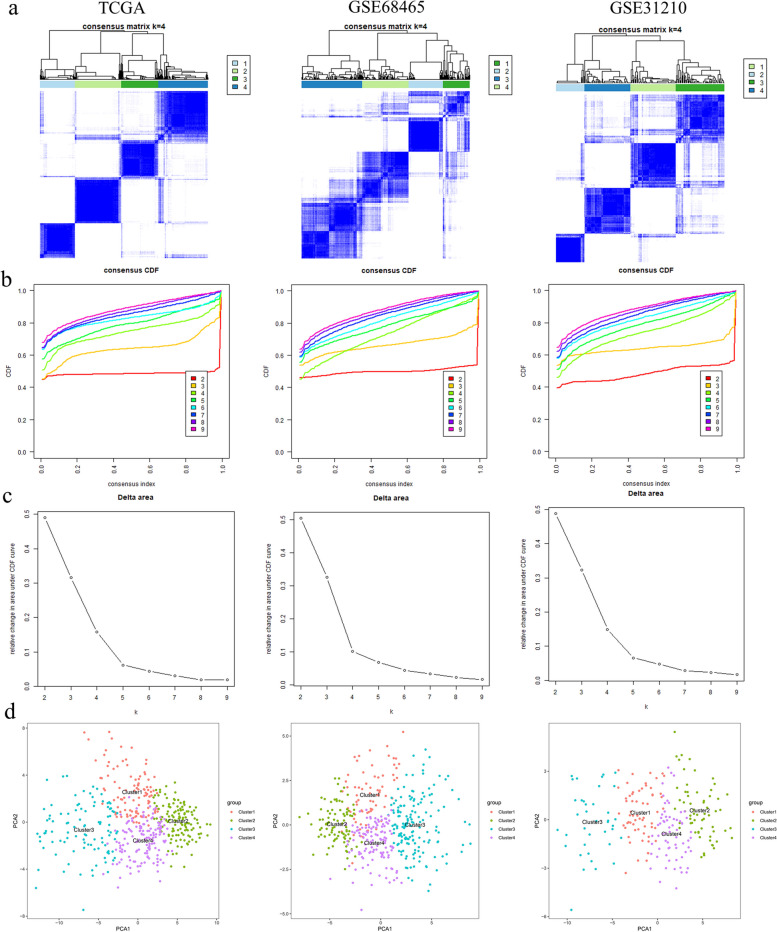
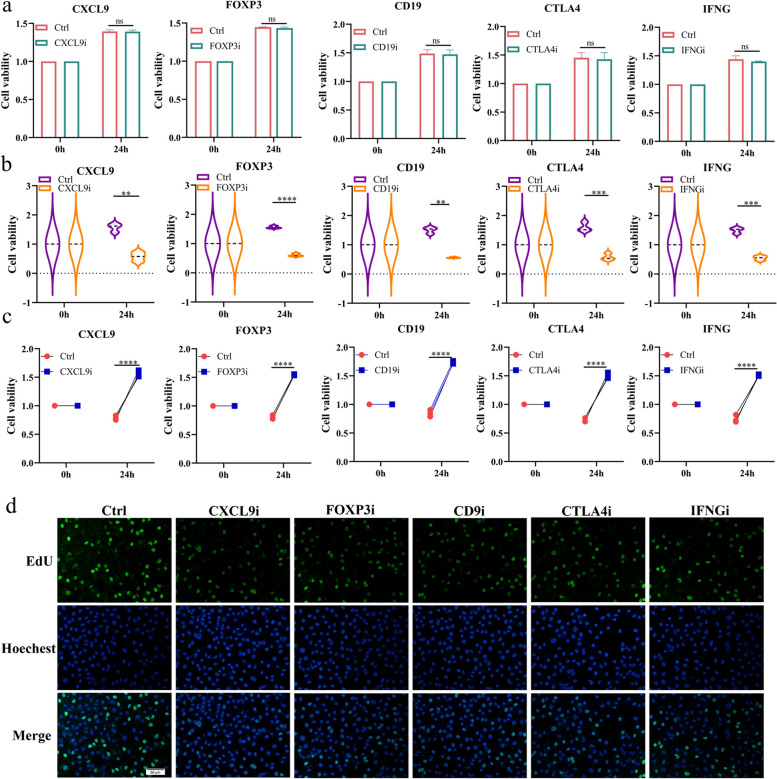
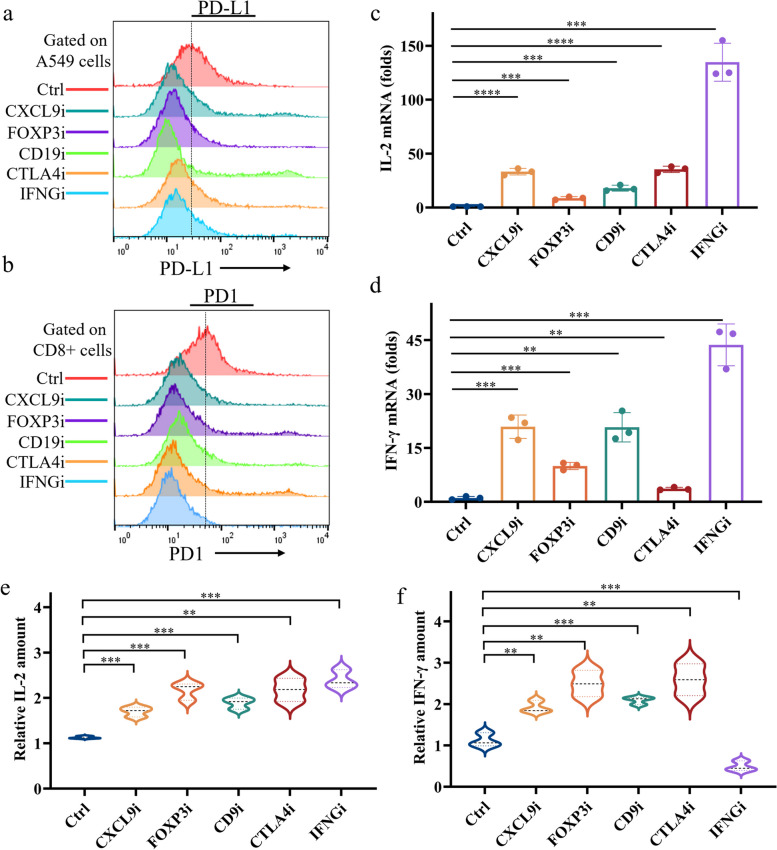
Methods: The differentially co-expressed genes associated with CD8 + T cells were identified through weighted gene co-expression network analysis (WGCNA) and the Search Tool for the Retrieval of Interacting Genes (STRING) database. These gene signatures facilitated consensus clustering for TCGA-LUAD and GEO cohorts, categorizing them into distinct immune subtypes (C1, C2, C3, and C4). The Tumor Immune Dysfunction and Exclusion (TIDE) model and Immunophenoscore (IPS) analysis were employed to assess the immunotherapy response of these subtypes. Additionally, the impact of inhibitors targeting five hub genes on the interaction between CD8 + T cells and LUAD cells was evaluated using CCK8 and EDU assays. To ascertain the effects of these inhibitors on immune checkpoint genes and the cytotoxicity mediated by CD8 + T cells, flow cytometry, qPCR, and ELISA methods were utilized.
Results: Among the identified immune subtypes, subtypes C1 and C3 were characterized by an abundance of immune components and enhanced immunogenicity. Notably, both C1 and C3 exhibited higher T cell dysfunction scores and elevated expression of immune checkpoint genes. Multi-cohort analysis of Lung Adenocarcinoma (LUAD) suggested that these subtypes might elicit superior responses to immunotherapy and chemotherapy. In vitro experiments involved co-culturing LUAD cells with CD8 + T cells and implementing the inhibition of five pivotal genes to assess their function. The inhibition of these genes mitigated the immunosuppression on CD8 + T cells, reduced the levels of PD1 and PD-L1, and promoted the secretion of IFN-γ and IL-2.
Conclusions: Collectively, this study delineated LUAD into four distinct subtypes and identified five hub genes correlated with CD8 + T cell activity. It lays the groundwork for refining personalized therapy and immunotherapy strategies for patients with LUAD.
Keywords: CD8 + T cells; Immune subtype; Immunotherapy response; Lung adenocarcinoma; PD-L1.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




Similar articles
-
Development of an immune-related gene signature applying Ridge method for improving immunotherapy responses and clinical outcomes in lung adenocarcinoma.PeerJ. 2025 May 8;13:e19121. doi: 10.7717/peerj.19121. eCollection 2025. PeerJ. 2025. PMID: 40352269 Free PMC article.
-
Identification of the molecular subtype and prognostic characteristics of lung adenocarcinoma based on CD8+ T cell-related gene signature.Cancer Biomark. 2024 Dec;41(3-4):18758592241296764. doi: 10.1177/18758592241296764. Epub 2025 Mar 17. Cancer Biomark. 2024. PMID: 40095496
-
Investigating subtypes of lung adenocarcinoma by oxidative stress and immunotherapy related genes.Sci Rep. 2023 Nov 27;13(1):20930. doi: 10.1038/s41598-023-47659-8. Sci Rep. 2023. PMID: 38017020 Free PMC article.
-
The role of B cell immunity in lung adenocarcinoma.Genes Immun. 2025 Jun;26(3):253-265. doi: 10.1038/s41435-025-00331-9. Epub 2025 May 13. Genes Immun. 2025. PMID: 40360749 Review.
-
Alternative Splicing in Lung Adenocarcinoma: From Bench to Bedside.Cancers (Basel). 2025 Apr 15;17(8):1329. doi: 10.3390/cancers17081329. Cancers (Basel). 2025. PMID: 40282505 Free PMC article. Review.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
